|
(Washington D.C.) — Moderna announced Monday that U.S. health regulators granted full approval to its COVID-19 vaccine, a shot that’s been given to tens of millions of Americans since its emergency authorization over a year ago. The action by the Food and Drug Administration means the agency has completed the same rigorous, time-consuming review of Moderna’s shot as dozens of other long-established vaccines. The decision was bolstered by real-world evidence from the more than 200 million doses administered in the U.S. since the FDA cleared the shot in December 2020. The FDA granted full approval of Pfizer’s vaccine last August. Public health advocates initially hoped the regulatory distinction would boost public confidence in the shots. But there was no discernible bump in vaccinations after the Pfizer approval, which was heavily promoted by President Joe Biden and other federal officials. More than 211 million Americans, or 63% of the total population, are fully vaccinated. About 86 million people have gotten a booster dose. Vaccinations peaked last spring at more than 3 million per day, and now average less than 750,000 per day. The pace of vaccinations briefly spiked following news of the omicron variant in December but has since slowed again. The FDA, like regulators in Europe and elsewhere, initially allowed emergency use of Moderna’s vaccine based on a study that tracked 44,000 people 18 and older for at least two months — the time period when serious side effects typically arise. That’s shorter than the six months of safety data normally required for full approval, so Moderna continued that study. The FDA also kept watch for serious side effects that have proved to be very rare. In the U.S., Moderna is used only by adults. The company said last fall that FDA had delayed deciding whether to clear the shots for 12- to 17-year-olds as it examined a rare risk of heart inflammation seen mostly in young men and teen boys. Johnson & Johnson has not yet applied for full approval of its COVID-19 vaccine. ___ AP Medical Writer Lauran Neergaard contributed to this report. from https://ift.tt/HiPO0jTdF Check out https://takiaisfobia.blogspot.com/
0 Comments
Opioid prescriptions have fallen in recent years, after health care providers became more aware of the risks of overdoses and the federal government tightened prescribing rules. While opioids were dispensed at a rate of 81 prescriptions for every 100 Americans in 2012, that rate dropped nearly in half by 2020, according to data from the U.S. Centers for Disease Control and Prevention. However, overdoses involving prescription opioids have remained high. In 2020, more than 68,000 overdose deaths in the U.S. involved an illicit or prescription opioid, up from about 21,000 in 2010, according to federal data. Researchers are trying to predict who is most at risk for having an opioid overdose—and they’re finding that some Americans face more danger than others. A new study published in JAMA Network Open has found that a person’s age, sex, race, insurance type, and more can all place them at greater risk. In the JAMA study, researchers looked at data for nearly 237,000 adults in Oregon who didn’t have a previous history of using opiates but who were prescribed them in 2015. They tracked the data for an additional three years and found that 667 people had fatal or non-fatal opioid overdoses during that time: a rate of about 3 in 1,000. This is a relatively high rate for a population without a prior history of opiate use, says Dr. Scott Weiner, study co-author and an associate professor of emergency medicine Harvard Medical School. “Just getting an opiate prescription is going to put you at risk for having an overdose.” Weiner and his team teased out several risk factors that seemed to put certain Oregon patients at higher risk for an overdose. Men, who are more likely than women to overdose on any kind of drug, were 29% more likely to overdose than women in this group; residents of metropolitan counties were 51% more likely to overdose than people who didn’t live in cities, and Black patients were 55% more likely to overdose than white patients. (However, the authors note that since nearly 87% of Oregon residents are white, this may not be representative of the whole country.) Being elderly seems to put people at an especially heightened risk. People ages 75 and older were about three times more likely to overdose than people ages 35 to 44. This is particularly worrisome because older adults are more vulnerable to overdose in several ways; they have a weaker ability to metabolize opiates than younger people, for one. Read More: U.S. Life Expectancy Dropped Nearly 2 Years in 2020 Using certain types of insurance was also linked to a greater likelihood of overdose. Patients with Medicaid or Medicare Advantage—an insurance plan offered by some private companies that serves as a replacement for Medicare—were more likely to overdose than people with commercial insurance. People who qualified for both Medicaid and Medicare Advantage were especially vulnerable, facing more than four times the risk of overdosing as people with commercial insurance. The type of insurance a person uses can signal whether they’re facing other risks—including food, housing, and job insecurity—which other research has shown also puts people at greater risk for overdose, Weiner says. “Social factors really do play a part in this as well,” he says. However, even people who are at higher risk of overdosing should not lose access to opioids when they have severe pain, Weiner says. Although opioid prescriptions are widespread in the U.S, some demographics have historically had inadequate access to them, including Black patients. In part, experts attribute this discrepancy to racism and bias among prescribers; health care providers have been shown to underestimate Black patients’ pain. What the new research instead suggests, Weiner says, is that both patients and prescribers should take steps to make sure they’re approaching opiates with caution, especially if patients have risk factors placing them at greater risk of an overdose. Health care providers can help reduce risk by taking certain precautions, Weiner says. One is to prescribe non-opioid medications whenever possible (or tell patients to use them once their pain subsides) and make sure that patients are educated about how to use opioids and dispose of them safely. When a patient has one or more risk factors—like those Weiner and his team identified—providers should consider spending more appointment time with them to make sure they know how to use the medication safely, or call them to check in following their visit, Weiner says. Providers can also use several tools in order to dispense these drugs more judiciously, including checking their states’ prescription drug monitoring programs to see patients’ prescription histories, and prescribing the smallest dosage possible that will adequately treat a person’s pain. Patients and their loved ones can help reduce overdose risk, too. Patients and their families should recognize that opioids are only meant to help with the worst pain and should be disposed of safely, like at a pharmacy, Weiner says. Families should also monitor the person taking opioids for signs of tolerance, dependence, or opioid use disorder—such as a patient refilling their prescription early, or using the drug differently than they were prescribed, says Weiner. If that happens, they should reach out to a prescriber to ask for help. “If they do fall into the higher risk factors, then that’s good for them to know,” says Weiner. “Because when they do get a prescription, they should be asking the prescriber how they can be safe with it.” from https://ift.tt/3INFxrW Check out https://takiaisfobia.blogspot.com/ As the Supreme Court weighs the high-profile case that could unwind Roe v. Wade—and, with it, the Constitutional right to abortion--conservative state lawmakers are introducing a wave of new bills aimed at limiting abortion at the state level. While several states have introduced bills mimicking Texas’ controversial six-week abortion ban, at least three more—Florida, Arizona and West Virginia—are considering laws that would ban abortion after 15 weeks of pregnancy, modeled on the Mississippi law at the center of the Supreme Court case. These bills directly violate the so-called viability standard set by Roe v. Wade, which states that women have the constitutional right to end pregnancies until the fetus is viable. But proponents are betting that the Supreme Court’s decision, which is expected before the end of June, will allow Mississippi’s 15-week ban to stand. They are arguing that the 15-week ban is a more reasonable alternative to the extreme, Texas-style laws that curtail access to abortion after about just six weeks. “I believe that we have a unique opportunity in the fact that the Supreme Court is considering 15 weeks right now, and this would allow Florida to save as many babies as possible as soon as possible after that decision is made,” Florida state Rep. Erin Grall, the lead sponsor of her state’s 15-week ban, said during a House subcommittee hearing on Jan. 19. If state lawmakers in Florida, Arizona and West Virginia pass these 15-week abortion bans, they will likely face immediate court challenges. But if the Supreme Court decision allows Mississippi’s law to stand, the laws would likely then be enforceable. Abortion rights advocates say the push to pass 15-week abortion bans is a political move to enact significant restrictions while the public is distracted by Texas and the Supreme Court’s coming decision. “The goal of the anti-abortion politicians who are passing these laws is not to ban abortion at 15 weeks,” says Julie Rikelman, litigation director at the Center for Reproductive Rights, who argued the Mississippi case before the Supreme Court in December. “The goal is to eliminate access to abortion entirely, to make it completely illegal—criminal—for people to be able to make this decision for themselves.” A Supreme Court-inspired strategyState lawmakers generally consider multiple bills aimed at curtailing abortion during every legislative session. And while it’s been relatively common for legislators to introduce measures banning abortion both early in pregnancy and later in pregnancy such as at 20 weeks, few states had previously focused on 15 weeks as a cut-off point. Before this year, Mississippi and Louisiana were outliers for their laws prohibiting abortion after the point of 15 weeks. In West Virginia, the bill’s lead sponsor Republican Del. Ruth Rowan, told West Virginia Public Broadcasting, “we need to start somewhere, and in saying that, Mississippi’s done it and we can do it too.” Another Republican Del. Kayla Kessinger, said that the bill was a direct preparation for the coming Supreme Court ruling. “States have a vested interest in determining what abortion should look like, when abortion should be available,” she told West Virginia MetroNews. “So why are we doing it now? We want the Supreme Court to know Mississippi isn’t the only state that wants to tackle this issue.” In Arizona and Florida, lawmakers have introduced both a 15-week ban and copycat bill of Texas’ SB 8, which bans abortion around six weeks and financially incentivizes private citizens to enforce it by suing anyone who they think has helped someone get an abortion after that point. In Florida, the 15-week bill has momentum in the state legislature. Advocates on both sides of the abortion issue have noted that the bills seem opportunistic rather than driven by ideology. “They’re trying to take the safest route politically possible instead of going and doing the right thing, which I believe is eliminating abortion as much as possible as early as possible in pregnancy, and hopefully, really from the moment of conception on,” says Andrew Shirvell, founder and executive director of Florida Voice for the Unborn. Shirvell strongly prefers the Texas copycat bill that he hoped would “cripple the abortion industry” in Florida, but that legislation does not have a companion bill in the Florida Senate, so will not likely pass this term. In recent years, Shirvell says he has been disappointed that Florida has not adopted more restrictions on abortion. But the Supreme Court “gave Florida legislators some more momentum in terms of trying to ban later term abortions here in Florida,” he says. Read More: Supreme Court Allows Texas Abortion Law to Stand, But Says Abortion Providers Can Challenge It On that point, abortion rights advocates agree. “I think it is politically motivated,” says Laura Goodhue, executive director of the Florida Alliance of Planned Parenthood Affiliates. Florida currently allows abortion up to 24 weeks, and she noted that one reason the state has enacted fewer restrictions than others around it is that Florida has a strict right to privacy in its state constitution. “However, the Florida State Supreme Court has also seen a turnover in judges that may not necessarily uphold that strong right to privacy. So I believe that politicians in Florida are trying to push that limit,” Goodhue says. A stepping stoneProponents of the 15-week bans are presenting them as a middle ground between more extreme measures and the current state of access. In Florida, conservative lawmakers noted that people would still be able to get abortions until 15 weeks or past 15 weeks if the pregnant person’s life is at risk or the fetus has a fatal abnormality. None of the 15-week bills that have been introduced make exceptions for pregnancies resulting from rape or incest. Shirvell says the Florida bill would “save up to 5,000 unborn babies every year from being aborted and that’s a very positive thing.” But, he said, the bill won’t have as significant an impact as he would like because the majority of abortions take place during the first trimester. “The 15-week abortion ban bill will not save the vast majority of unborn children in Florida,” he says. Gov. Ron DeSantis told reporters earlier this month that a 15-week ban “makes a lot of sense” and that while he had not yet looked at this particular bill, he would likely sign it. “Obviously I’m supportive of 15 weeks. I mean, I think that’s very reasonable and I think that’s very consistent with, you know, being supportive of protecting life,” he told reporters on Jan. 12. This rang alarm bells for abortion rights supporters. In December, Rikelman told the Supreme Court that if the justices eliminated the viability standard and allowed Mississippi’s 15-week law to stand it would open the door to states trying to ban abortion at many other stages too. Rikelman says this recent wave of new 15-week bans is in line with what she predicted. “It’s really not a compromise,” she says. “It would just be devastating to the people who need access to abortion after 15 weeks.” ‘A domino effect’Prohibiting abortion at 15 weeks would fundamentally reshape abortion access in any state, but in Florida, Arizona and West Virginia, where many people live in rural communities, it could have especially significant consequences. “We know that whenever bans like the 15-week ban are enacted, they fall hardest on people of color, low income people, people living in rural areas, and young people—folks who are already marginalized by our health care system,” says Katie Quinonez, executive director of Women’s Health Center of West Virginia, the state’s only abortion clinic. West Virginia currently prohibits abortions after 20 weeks and requires patients to receive state-directed counseling and wait 24 hours before their abortion. For minors, their parents must be notified if they are getting an abortion. Read More: Inside Mississippi’s Last Abortion Clinic—and the Biggest Fight for Abortion Rights in a Generation Many people who want an abortion have to delay their care because they need to raise or borrow the money, take time off work, arrange transportation, find child care and figure out other logistics before they can make it to a clinic, Quinonez says. Others might not know they are pregnant right away or experience a change in their circumstances and then need to overcome those hurdles. Florida currently offers more access to abortion than most of the states surrounding it in the South. About 30% of patients at Planned Parenthood’s Tallahassee and Jacksonville locations have been from out of state in the last few years, according to Goodhue, and Florida clinics have seen a large influx of patients from Texas following the Lone Star state’s passage of SB 8 last fall. “The space in between has so many restrictions with very few providers. So it really does impact the entire country,” Goodhue says. If West Virginia implements its ban, the Guttmacher Institute, a research center that supports abortion rights, estimates the average one-way driving distance for someone seeking an abortion after 15 weeks would increase 59 miles or 90%. In Arizona, the driving distance would increase 282 miles or 2,459%, and in Florida, the distance would increase 570 miles or 4,443%. “It’s the people that have the means to travel to another state who get care, but then those states will also be inundated with appointments,” Goodhue says. This can create a “domino effect,” Rikelman adds. When one state passes new restrictions, that often forces patients to wait longer to get an abortion, meaning they may need to travel to another state. And if neighboring states see longer waiting lists, then residents there may also have to delay their abortions if appointments aren’t available immediately. “The more states curtail access to abortion, the harder it becomes for people in the entire region to access it,” Rikelman says. “Fifteen weeks is not the stopping point.” from https://ift.tt/3IQyuyV Check out https://takiaisfobia.blogspot.com/ Even as SARS-CoV-2 gets better at spreading and evading some of the immune protection that people have built through infections or vaccination, new variants inevitably arise. The latest is BA.2, a new version of Omicron. It’s too early to predict what BA.2 might mean for the course of the COVID-19 pandemic. But detecting such variants early will help public health experts better identify which ones pose the most danger to people’s health, and therefore require more stringent mitigation measures. Here’s what we know so far. What is the BA.2 variant?BA.2 appears to be a descendant of Omicron (which researchers are now referring to as BA.1). Researchers at the World Health Organization reported increasing numbers of BA.2 infections in January in Denmark, India, and the U.K. Even though it’s been just a few days since the variant was identified, South Africa and the U.S. have also reported cases of BA.2. So far, the virus has been detected in four U.S. states: California, New Mexico, Texas, and Washington. Scientists found BA.2 thanks to more widespread genetic sequencing, which is helping them detect changes in SARS-CoV-2 more quickly and determine how those mutations might affect human health. Is the new BA.2 variant more dangerous than Omicron?Like Omicron, BA.2 contains numerous mutations, according to researchers at the Massachusetts Consortium on Pathogen Readiness, a collaboration of academic researchers from different institutes in the Boston area who monitor genetic changes in SARS-CoV-2. About 20 mutations have been located in the antibody-binding regions that vaccines target. BA.2 also contains some mutations not found in BA.1, but scientists aren’t sure yet what those changes mean. Should you be worried?The WHO has not determined yet whether BA.2 as a variant of concern. So far, there isn’t enough information to determine how transmissible or virulent BA.2 might be, although in South Africa, BA.2 is now more prevalent than BA.1. It’s not yet clear whether BA.2 is more transmissible than Omicron. Will the current COVID-19 vaccines work against BA.2?It’s still unknown, but the good news is that there is growing evidence that vaccines generate both immediate and longer lasting immunity against all variants of SARS-CoV-2 so far. The antibodies that the shots catalyze may only protect against infection for a relatively short amount of time—Moderna reported this week that even after a booster dose of its vaccine, these virus-neutralizing antibodies tend to wane after six months—but the body’s immune response to vaccination also includes T cells. These are more durable and are aimed at more conserved regions of the virus; T cells seem to provide good and lasting protection against severe disease from every variant so far, even if people do get infected. from https://ift.tt/3IPQSYJ Check out https://takiaisfobia.blogspot.com/ WASHINGTON — The Environmental Protection Agency announced a series of enforcement actions Wednesday to address air pollution, unsafe drinking water and other problems afflicting minority communities in three Gulf Coast states, following a “Journey to Justice” tour by Administrator Michael Regan last fall. The agency will conduct unannounced inspections of chemical plants, refineries and other industrial sites suspected of polluting air and water and causing health problems to nearby residents, Regan said. And it will install air monitoring equipment in Louisiana’s “chemical corridor” to enhance enforcement at chemical and plastics plants between New Orleans and Baton Rouge. The region contains several hotspots where cancer risks are far above national levels. The EPA also issued a notice to the city of Jackson, Mississippi, saying its aging and overwhelmed drinking water system violates the federal Safe Drinking Water Act. The order directs the city to outline a plan to “correct the significant deficiencies identified” in an EPA report within 45 days. In separate letters, Regan urged city and state officials to use nearly $79 million in funding allocated to Mississippi under the bipartisan infrastructure law “to solve some of the most dire water needs in Jackson and other areas of need across Mississippi.” The actions were among more than a dozen steps announced being taken in response to Regan’s tour last November. Regan visited low-income, mostly minority communities in Mississippi, Louisiana and Texas as part of an effort to focus federal attention on communities adversely affected by decades of industrial pollution. A Toxics Release Inventory prepared by the EPA shows that African Americans and other minority groups make up 56% of those living near toxic sites such as refineries, landfills and chemical plants. Negative effects include chronic health problems such as asthma, diabetes and hypertension. “In every community I visited during the Journey to Justice tour, the message was clear: residents have suffered far too long and local, state and federal agencies have to do better,” Regan said. The unannounced inspections of chemical plants and other sites “are going to keep these facilities on their toes,” he told reporters on a conference call. Inspections currently are done on a schedule or with advance notice, Regan said, but that is about to change. “We are amping up our aggressiveness to utilize a tool that’s in our toolbox that … has been there for quite some time,” he said. When facilities are found to be noncompliant, the EPA “will use all available tools to hold them accountable,” he added. A pilot project combining high-tech air pollution monitoring with additional inspectors will begin in three Louisiana parishes—St. John the Baptist, St. James and Calcasieu—that are home to scores of industrial sites and are long plagued by water and air pollution. President Joe Biden has made addressing racial disparities, including those related to the environment, central to his agenda. He has pledged that at least 40% of new spending on climate and the environment go to poor and minority communities. The administration’s commitment to the issue has come under renewed scrutiny in recent weeks, as two key environmental justice appointees departed. Cecilia Martinez, a top official at the White House Council on Environmental Quality, and David Kieve, who conducted outreach with environmental justice groups, both left the White House, putting a spotlight on promises yet to be fulfilled. Regan, a former environmental regulator in North Carolina, has made environmental justice a top priority since taking over as EPA head last year. As the first Black man to lead the agency, the issue “is really personal for me, as well as professional,″ he told The Associated Press in November. “I pledge to do better by people in communities who have been hurting for far too long,” he said Tuesday. Historically marginalized communities like St. John and St. James, along with cities such as New Orleans, Jackson and Houston, will benefit from the $1 trillion bipartisan infrastructure law signed by Biden, Regan said. The law includes $55 billion for water and wastewater infrastructure, while a sweeping climate and social policy bill pending in the Senate would pump more than twice that amount into EPA programs to clean up the environment and address water and environmental justice issues. As part of its enforcement action, the EPA is requiring a former DuPont petrochemical plant in La Place, Louisiana, to install fence-line monitors to identify emissions from the site, Regan said. The plant is now owned by the Japanese conglomerate Denka. The agency also said it will push for greater scrutiny of a proposed expansion of a Formosa Plastics plant in St. James and issued a notice of violation to a Nucor Steel plant that emits hydrogen sulfide and other harmful chemicals. Regan said he has spoken with New Orleans Mayor LaToya Cantrell about Gordon Plaza, a city neighborhood built on the site of a former toxic landfill. Gordon Plaza was designated as a Superfund site in the 1990s, but dozens of mostly Black families still live there. The EPA will review the site, starting in March, Regan said, and will add nine homes not included in earlier plans to help families move. City officials hope to use money from the infrastructure law to relocate families and build a solar farm on the site. EPA also said it has completed a review of proposed actions to clean up creosote contamination from a site in Houston now owned by Union Pacific Railroad. The site, in the Kashmere Gardens area in the city’s Fifth Ward, has been linked to higher than normal cancer rates in the historically Black neighborhood. EPA said it will work with Texas officials to ensure corrective actions address the concerns of community members. Houston Mayor Sylvester Turner, who toured the area with Regan, said Wednesday it was “very encouraging” that federal officials “share our concerns and know the names and faces of those affected.” Sharon Lavigne, president of Rise St. James, a grassroots organization that has battled petrochemical plants in Louisiana, said the EPA’s actions were “just the beginning of what needs to be done” to address pollution from the petrochemical industry. “It’s important that EPA recognizes the need to listen to the science, which shows the destructive Formosa plastics facility should be stopped and that no other harmful chemical facilities should be allowed to cause harm in our community anymore,” Lavigne said. “I’m hopeful that he will really get some things done.” from https://ift.tt/3r5elir Check out https://takiaisfobia.blogspot.com/ The gas-burning stoves loved by cooks leak so much methane across the U.S.—most when the appliances are not even in use—that they have the same impact on our atmosphere as half a million cars, according to a Stanford University study. Stanford researchers analyzed indoor levels of both heat-trapping methane and nitrous oxides—pollutants that can trigger asthma and other breathing problems—and found surprising amounts of each seeping from stoves. The study, released Thursday, comes as communities nationwide debate whether to ban natural gas use in new buildings as part of the fight against climate change, and as the gas industry mobilizes to block such bans. “Gas stoves warm the planet and release indoor air pollutants that you breathe–you get both,” senior author Rob Jackson, an environmental scientist at Stanford, said in an interview. Eliminating gas service for newly built homes makes sense, he said, “otherwise we’re locking in greenhouse gas emissions for decades to come.” Methane, the main component of natural gas, has more than 80 times the global-warming potential of carbon dioxide for the first 20 years after it’s released into the atmosphere. The study, which measured methane levels in 53 California home kitchens sealed off with plastic sheeting, found that old and new stoves alike leak the gas, with 76% of the emissions happening while the appliances aren’t used. Since more than one-third of U.S. households, or 40 million homes, have gas-burning stoves, the researchers estimate their nationwide methane emissions each year have the same global-warming potential as about 500,000 cars. The study also examined levels of nitrous oxides in 32 of the kitchens and found that while stoves are in use, levels of the pollutants can exceed federal exposure guidelines if the kitchens don’t have ventilation hoods or those hoods aren’t switched on. It isn’t clear how much methane is coming from leaky pipes and fittings, incomplete combustion of the gas, design features of the stoves or a combination of those factors. The researchers would like to expand the study to include more homes and stoves, since the pandemic limited testing. Tests involved sealing off part of each kitchen to avoid emissions from gas-burning furnaces or water heaters elsewhere in the house. The researchers worked with real estate agents to find empty homes or rented them on Airbnb. The study included 18 brands of stoves, ranging in age from 3 to 30 years. “The trickier question is how to swap out older stoves,” Jackson said. “I would hope for all the readers, their next stove is electric, no matter when they buy it.” from https://ift.tt/3rTJZP6 Check out https://takiaisfobia.blogspot.com/ Moderna reported today the first data on how well its currently authorized vaccine and booster hold up against the Omicron variant, which quickly dominated new infections around the world after health experts first described the variant last November. The company also announced that it is starting to study its Omicron-specific vaccine. In a correspondence published in the New England Journal of Medicine, the company’s scientists reported the results of a study involving blood samples from a small number of vaccinated participants. Antibody levels generated by Moderna’s primary two-dose regimen continued to neutralize Omicron in lab tests, but these levels were 35 times lower against Omicron than the original SARS-CoV-2, against which the vaccine was designed. A booster dose of the vaccine—which is half of one dose of the original shot—increased antibody levels in 20 study participants to 20 times higher than levels generated after the second dose of the vaccine, therefore restoring some of the waned protection. The scientists also tested a booster at the same dose as the primary two doses in another 20 volunteers, and that booster produced antibody levels that were at least two times higher than those generated by the half-dose booster. Currently, however, the U.S. Food and Drug Administration has authorized only the half-dose booster of Moderna’s shot, based on data before Omicron emerged that the half dose elicited similar antibody levels against previous variants as another full-dose booster. Read More: We Urgently Need a New National COVID-19 Response Plan These antibodies against Omicron started to wane after about six months, the company reported. After hitting a peak about a month after the booster, neutralizing antibody levels dropped 6.3 fold; even more concerning, this decline occurred more quickly than the decline against the original virus that the vaccine targeted. Such rapid waning of protection after boosting with the existing vaccine makes a strong case for potentially boosting with an Omicron-specific shot, which the company is studying. That trial will include 300 people in 24 sites across the U.S. (This week, Pfizer and BioNTech also announced that they have started testing an Omicron-specific vaccine.) Moderna’s scientists are also evaluating combination vaccines, in which they put together vaccines developed for different variants, including one that targets the original virus and one that targets Omicron. Such a cocktail approach may provide broader, more durable protection against COVID-19. from https://ift.tt/3IIYkVA Check out https://takiaisfobia.blogspot.com/ The recent Chicago public school crisis, collapse of Broadway theater in New York City, ongoing changes in NBA and NFL screening protocols for players, and extreme scarcity of rapid tests throughout the nation all serve as a deafening wake-up call for urgent revision of our national COVID-19 response plan. These and similar scenes of chaos and conflict over the reopening of American institutions and commerce reflect the absence of a coherent national plan that is responsive to the contagiousness of the Omicron variant. Central to this current failure is the need for a clear national definition of “public safety” that the American people can understand and buy into. Vague and impressionistic appeals to “safety” are riven by partisan divisions over real-world policy and implementation. First, we must fix this definition of safety as the necessary foundation to building a robust national plan. Second, our COVID-19 policies should not abruptly lurch from scientific study to study, changing availability of vital tools, and move from federal agency to agency. Rather policies must pragmatically respond to motivators of human behavior and to a coherent view of where the pandemic is headed. The new plan must face into current political realities.The best single predictor of Americans’ response to the pandemic has been their political ideology and partisanship. Polling throughout the pandemic has consistently revealed a deep Red State/Blue State polarization in COVID-related attitudes, behaviors and policies. Significant differences in immunization and death rates are also noted across party lines at both the state and county levels. This becomes especially relevant when considering that over the past year there was a 17 to 20-fold increase in the hospitalization and mortality rates in unimmunized versus immunized populations. The Omicron variant’s communicability and rapid spread has further exacerbated these divisions. Most states are currently experiencing their highest yet pandemic caseloads, though starting to decline in some places. Health systems and providers are overwhelmed and burned out. At the same time schools, colleges, employers, and most segments of society are struggling to “return to normal” as they contend with pushback from key constituents over the definitions and markers of safety. As a nation we are stagnating because we simply haven’t come to grips with what we need to do. Dr. Anthony Fauci, the President’s chief medical advisor, has recently championed, “we have to get the American people to pull together.” But patriotic appeals for bipartisan harmony are woefully insufficient to unite us. To restore our dynamism and prosperity we must forge a new national COVID-19 plan based on a pragmatic application of public health principles that encompasses both of our familiar political counter-narratives. The liberal narrative calls for infection-avoidance at all cost and is more willing to accept socioeconomic consequences of personal and societal safety measures. Conservatives tend to have a higher risk tolerance for infection and are more willing to accept its health consequences for themselves and the public. Read More: Omicron Could Be the Beginning of the End of the Pandemic Bipartisan policymaking must be evidence-driven and responsive to both political narratives. Neither counter-narrative has a monopoly on “following the science.” Omicron is politically agnostic. While the virus is blind to religion, ethnicity, race and gender, it does render the economically disadvantaged and those with underlying health conditions highly vulnerable. It also has a fierce geriatric agenda. This leads to an aspirational but achievable framework for a new national policy with four pillars responsive to Omicron’s now reasonably well-defined characteristics: 1) Change the national policy goalpost for the non-vulnerableOur present goal is to avoid cases or infections—defined as test positives—in everyone. With the unprecedented communicability and relatively mild health outcomes of Omicron this is unsustainable and unnecessary. The new foundation and lynchpin of our national goal must be serious health outcomes (ER visits, hospitalizations and deaths) in the 260 million non-vulnerable Americans. A University of Washington review of recent studies and modeling concludes that Omicron is 90-99% less severe than Delta. This is due to a large increase in asymptomatic infections (about 80-90 percent of total), a 50 percent reduction of those who are symptomatic being hospitalized, and of those hospitalized a 5-10 fold reduction in dying. These numbers put the relative risk of serious illness from Omicron in the non-vulnerables in the same ballpark as the flu, a virus we have learned to live with. Many non-vulnerables equate infection with fear of dying, debilitating long-term effects, and jeopardizing the safety of loved ones. These emotions are deeply-ingrained from two years of fear. This is frequently reinforced by emphasis on alarming uncertainties by our public health officials, scientists, mainstream and social media. This does not reflect a balanced data-driven risk assessment. Important concerns should be addressed by focusing on protecting the vulnerable. A robust nationwide public education campaign to build confidence in this strategy and to address fear, misconceptions and relative risk must accompany movement of the goalpost to focus on serious outcomes. The longer we delay in making this inevitable political and cultural transition in resetting our goals from avoiding infections to avoiding serious disease, the longer this political bifurcation and conflict will continue to hamstring us. 2) Focus public health and social protection on the most vulnerableEighty percent of America’s COVID-19 deaths and 46 percent of hospitalizations are concentrated in older people and the immunocompromised. Over-65’s have a 95% full vaccination rate and more than half have received a booster, but they are still at risk for breakthrough infections and serious outcomes. This population continues to absorb the brunt of the pandemic’s wrath and every effort should be in place to mitigate their risk. With Omicron’s risk profile, avoiding infection is an obligatory common sense mitigation strategy only in the vulnerable population. In congregate facilities this means avoiding exposure through mandatory vaccination and rapid screening of staff and guests. We must also ensure their ready access to the remarkably effective new oral anti-viral therapies. It’s more difficult to ensure these protections in multigenerational households and public indoor settings, and this merits further consideration of housing and other indoor mitigation best practice. 3) Maximize voluntary vaccine uptake while minimizing mandates.Vaccination is strongly protective against serious consequences caused by Omicron. Yet about 39 million Americans remain highly resistant to being vaccinated. Nearly everyone will become at least partially immune in the current surge through vaccine or natural infection-generated immunity. When the unvaccinated become infected they passively provide further public good benefit in slowing transmission—although the amount can vary considerably across individuals. Immunization policy should consider the marginal cost-benefit of general mandates under these circumstances. The public health risk that unvaccinateds present to vulnerables should be the major driver of vaccine mandates. Policy mandates should be applied in a more targeted way focusing on high priority public health impact (eg. nursing homes and health care workers). We should avoid mandates in settings where the political friction outweighs the public health benefit. 4) Re-cast the role of preventive interventionsPolicies involving masking, physical distancing, quarantine, self-isolation, and screening and surveillance testing should be re-examined to align with the new goalposts. Public policy should mandate these interventions only where interruption of transmission is of clear public health benefit in high-risk settings—defined as those directly affecting vulnerable people—such as public transport, congregate facilities and multi-generational households. The role and indications for routine rapid testing and surveillance of asymptomatic populations should be closely evaluated. Personal and institutional choice should be allowed to govern use of these preventive interventions in non-high risk settings. Omicron’s ubiquity and much lower virulence has given us the biological signal to move on to the inevitable endemic “living with the virus” endgame. The country must now challenge itself in both the public policy and personal realm to heed its implications. Omicron has presented us with clear new bipartisan goalposts: prevent serious outcomes in 260 million non-vulnerable Americans, and infections in the remaining 70 million. Our job now is to get the ball in the end zone. from https://ift.tt/3o2M8qv Check out https://takiaisfobia.blogspot.com/ (New York) — The COVID-19 booster drive in the U.S. is losing steam, worrying health experts who have pleaded with Americans to get an extra shot to shore up their protection against the highly contagious Omicron variant. Just 40% of fully vaccinated Americans have received a booster dose, according to the Centers for Disease Control and Prevention. And the average number of booster shots dispensed per day in the U.S. has plummeted from a peak of 1 million in early December to about 490,000 as of last week. Also, a new poll from The Associated Press-NORC Center for Public Affairs Research found that Americans are more likely to see the initial vaccinations—rather than a booster—as essential. “It’s clear that the booster effort is falling short,” said Jason Schwartz, a vaccine policy expert at Yale University. Overall, the U.S. vaccination campaign has been sluggish. More than 13 months after it began, just 63% of Americans, or 210 million people, are fully vaccinated with the initial rounds of shots. Mandates that could raise those numbers have been hobbled by legal challenges. Vaccination numbers are stagnant in states such as Wyoming, Idaho, Mississippi and Alabama, which have been hovering below 50%. In Wyoming, 44% are fully vaccinated, up just slightly from 41% in September. To boost numbers, the state has been running TV ads with health care workers giving grim accounts of unvaccinated people struggling with COVID-19. “Certainly we would like to see higher rates. But it would be wrong for anyone to think that the rates we have are due to lack of effort,” Wyoming Health Department spokeswoman Kim Deti said Tuesday. Read More: Vaccine Scientists Are TIME’s 2021 Heroes of the Year And in neighboring Idaho, which also has one of the country’s lowest vaccination rates, the number of people getting their first vaccine dose has remained under 1,000 almost every day this year and the number getting booster shots is also declining. Still, officials say they won’t give up. “I don’t like to use the word ‘resigned,’” said Elke Shaw-Tulloch, administrator of the Idaho Division of Public Health. “I think we just need to keep saying it over and over again, how important it is.” At the other end of the spectrum, Vermont is a national leader in the percentage of people who have been fully vaccinated and received a booster shot. About 60% of the population over 18 has gotten a booster. But it’s not enough, said Vermont Health Commissioner Mark Levine. “I’d love to see that percentage much closer to 90%,” Levine said. The U.S. and many other nations have been urging adults to get boosters because the vaccine’s protection can wane. Also, research has shown that while the vaccines have proved less effective against Omicron, boosters can rev up the body’s defenses against the threat. As for why an estimated 86 million Americans who have been fully vaccinated and are eligible for a booster have not yet gotten one, Schwartz said public confusion is one important reason. “I think the evidence is now overwhelming that the booster is not simply an optional supplement, but it is a foundational part of protection,” he said. “But clearly that message has been lost.” The need for all Americans to get boosters initially was debated by scientists, and at first the government recommended only that certain groups of people, such as senior citizens, get additional doses. The arrival of omicron, and additional evidence about falling immunity, showed more clearly a widespread need for boosters. But the message “has been lost in the sea of changing recommendations and guidance,” Schwartz said. The AP-NORC Center poll found that 59% of Americans think it is essential that they receive a vaccine to fully participate in public life without feeling at risk of COVID-19 infection. Only 47% say the same about a booster shot. Keller Anne Ruble, 32, of Denver, received her two doses of the Moderna vaccine but hasn’t gotten her booster. She said she had a bad reaction to the second dose and was in bed for four days with a fever and flu-like symptoms. “I believe in the power of vaccines, and I know that’s going to protect me,” said Ruble, the owner of a greeting card sending service. But the vaccine “just knocked me out completely and freaked me out about getting the booster.” She said she does plan to get the booster in the next few weeks and in the meantime wears an N95 mask and tries to stay home. “I just don’t want to get COVID in general,” she said. “It does scare me.” Blake Hassler, 26, of Nashville, Tennessee, said he doesn’t plan to get the booster. He received Pfizer’s two doses last year after having a mild case of COVID-19 in 2020. He said he considers himself to be in a low-risk category. “At this point, we need to focus on prevention of serious illness at the onset of symptoms rather than creating a new shot every six weeks and more divisive mandates,” he said. ___ AP writers Mead Gruver in Fort Collins, Colorado; Wilson Ring in Montpelier, Vermont; Rebecca Boone in Boise, Idaho, and Mike Stobbe in New York contributed to this report. from https://ift.tt/33TZu1A Check out https://takiaisfobia.blogspot.com/ When Jeremy Luban first looked over the genetic sequence of the Omicron variant on his phone one day last November, it was five o’clock in the morning. But even at that hour, the University of Massachusetts virus expert knew right away Omicron was a problem. First, there was the sheer number of new mutations—by some counts, as many as 50, with 30 of them in the critical places that vaccines and drug treatments target. Second, this new version of the SARS-CoV-2 virus seemed to appear out of nowhere, unpredictably and with no immediately obvious connection to previous variants. “It’s like when you look at the first page of a comic book and all of the Marvel villains have gotten together,” he says. “That was literally what it was like when I saw the sequence. How are we going to survive this? We can deal with one [mutation], but 10 or more of them all at once?” Other public health officials shared Luban’s alarm, but, it turns out, Omicron, like all villains, has an Achilles’ heel. For people who are vaccinated or who have been exposed to its predecessors, this variant does not seem to cause severe disease. While it can still be dangerous for people who are unvaccinated, or who have health conditions that make them more vulnerable to COVID-19’s effects, for the vaccinated, there was a glimmer of hope. Whether justified or not, that glimmer has been flamed into a blazing beacon by some people, who interpret Omicron’s relatively mild effect on health if you’re vaccinated—a sore throat, some flu- or cold-like symptoms, or no noticeable symptoms at all—as a sign that SARS-CoV-2 may be reaching the end of its onslaught. If Omicron isn’t as virulent, then SARS-CoV-2 must be weakening, the thinking goes. Even leading scientists have been tempted by the idea, admitting that of all the versions of SARS-CoV-2 that have hit humanity over the past two years, Omicron might be the preferable one to get infected with, since it doesn’t make the immunized that sick. And if more vaccinated people are infected with Omicron and develop immunity, that protection, combined with the protection that some people might have from being infected with previous variants, could reach the magical herd immunity threshold—which experts say could be anywhere between 70%-90% of people recovered from or vaccinated against COVID-19—that would finally make SARS-CoV-2 throw up its spike proteins in defeat. Read more: No, You Should Not Try to Get Omicron According to some models, by the time Omicron works its way through the population, up to half of people around the globe will have been infected, and presumably immune to the variant. With fewer unprotected hosts to infect, viruses generally begin to peter out—epidemic influenza viruses are a good example—and optimistic models show that after a peak of cases by the end of January and beginning of February, SARS-CoV-2 may follow that path. Under that assumption, COVID-19 would begin its shift from being a pandemic disease to an endemic one, confined to pockets of outbreaks that erupt among immunocompromised populations or the unvaccinated, such as the youngest kids—but are manageable and containable because most people would be protected from the worst effects of the virus. But there’s also the possibility of a darker timeline, in which the unpredictable nature of SARS-CoV-2 to date drives the next year and beyond. If that occurs, it could mean the sobering possibility that Omicron is not the beginning of the end, but just the beginning of a more transmissible, more virulent virus that could do even more harm than it has already. Scenario #1: The COVID-19 virus has achieved equilibrium with humansLet’s start with the more sanguine prediction of what 2022 might hold for SARS-CoV-2. There are several lines of scientific evidence that support this perspective, including some long-held truisms about how viruses behave as they find more hosts to infect. Viruses mutate every time they make copies of themselves, becoming more or less infectious, or more or less harmful to their hosts. For a changing virus, it’s all about balance; finding the right mutations that allow it to become more efficient at spreading from one host to another in order to infect cells, while not causing so much disease that the host dies. A dying or dead host won’t help it to keep replicating. Textbooks teach that viruses, being the relatively simple entities that they are, have limited resources to devote to their one goal: survival. A virus can’t even reproduce on its own, and needs to borrow the reproductive machinery of cells from those that it infects. So, when a genetic mutation makes a virus more adept at spreading from one host to another, with each new host a brand new virus-making factory, it’s a huge advantage. It also suggests that the virus is opting for transmissibility over virulence; it’s in its best interest to spread more quickly and replicate than in causing its host to die. 
Omicron appears to be the perfect example of that strategy. What Luban saw in the virus’s genetic sequence last November was a series of changes that made the variant at least several-fold more transmissible than the previous one, Delta, which was already twice as transmissible as the original version of SARS-CoV-2. Such high transmissibility led to Omicron’s quick dominance across the globe—replacing the previous variant, Delta, in a mere two months. “The speed with which Omicron took over was really amazing,” says Shangxin Yang, assistant professor of pathology and laboratory medicine at University of California Los Angeles. “It’s almost magical. In two weeks, it went from accounting for 1% of COVID-19 cases around the world to 50% of cases, and in one month, to almost 100% of cases. That’s amazing speed; we could never have imagined any virus could do that.” 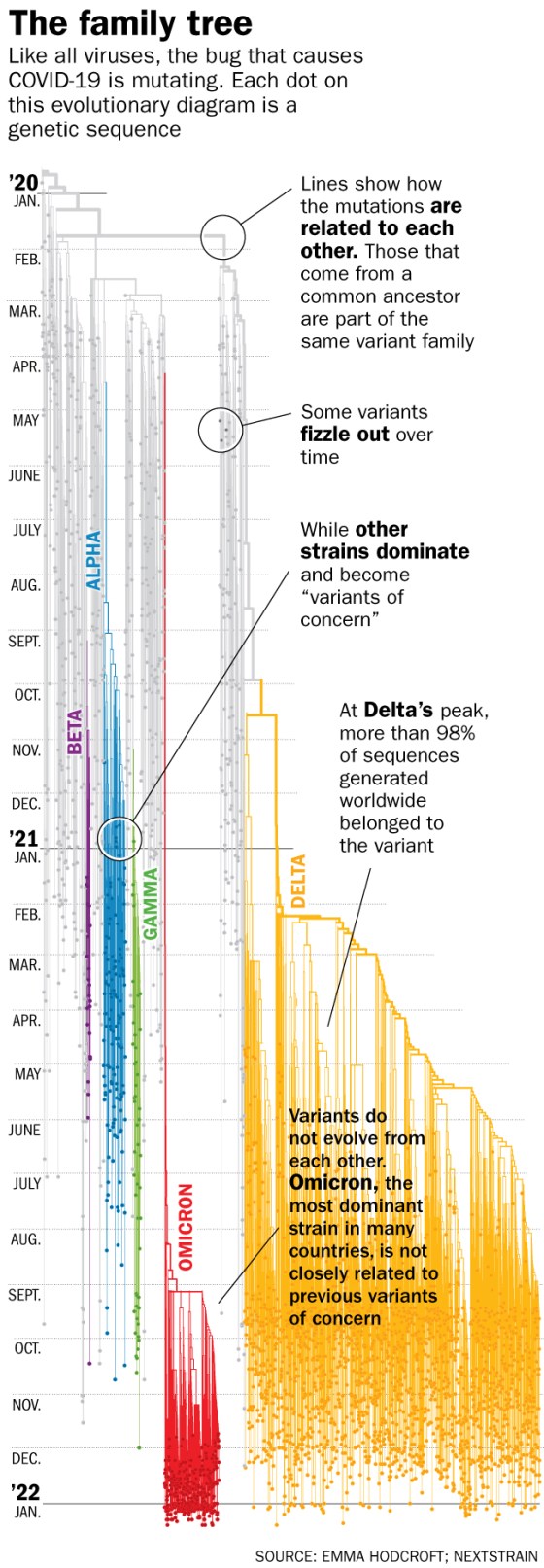
Yang points to other lines of evidence that suggests Omicron’s high transmissibility may herald SARS-CoV-2’s last hurrah. Whereas all previous variants of the virus preferentially infected cells deep in the human respiratory tract, nestling all the way into the lungs, Omicron tends to infect the cells in the upper respiratory tract. That makes it more like the common cold, and could explain why, at least among the immunized, Omicron tends to cause milder disease than previous variants. Read more: What Actually Worries U.S. Doctors About Omicron Those early versions of SARS-CoV-2 also tended to cause a phenomenon called cell fusion, in which a virus infects one cell, then co-opts other viruses that have infected other cells to fuse into a large viral mass to make a larger virus-making machine. That’s good for the virus, but bad for the patient, as it can trigger inflammation, which can in turn destroy cells and tissues; such inflammation is the hallmark of late-stage, severe COVID-19 disease. Omicron doesn’t lead to such cell fusion and therefore tends to cause less cell damage, which could in part explain, at least in immunized people, why those infected with Omicron tend not to get as sick. Recent data from the U.K. shows that vaccinated people infected with Omicron are two-thirds less likely to be hospitalized than vaccinated people infected with Delta. “All of this comes together to make the perfect scenario to end the pandemic,” says Yang. “This is exactly how most other pandemics with respiratory pathogens had ended. They spread like fire and then eventually most people either became vaccinated or infected and when the population reached herd immunity, the pandemic ended.” That doesn’t mean it’s the end of SARS-CoV-2, but it could signal the end of its pandemic phase. From there, COVID-19 should shift into being endemic, in which we learn to live with a virus that has already learned to live with us. Read more: We Need to Start Thinking Differently About Breakthrough Infections At this stage, says Yang, “the virus has already accomplished its goal of establishing a balance with its host—humans. It can spread easily among hosts, but not kill them, so it lives among its hosts. The virus has mutated to the point where it just chooses to live among us without causing too much trouble. And in return, we have to learn to live with the virus as if it is just another common cold.” That’s not just wishful thinking, he says—there’s historical precedent. Already, there are four coronaviruses that have been circulating among us for decades causing mild symptoms similar to the common cold. At some point in history, these coronaviruses could, hypothetically, have burned through the world’s population like SARS-CoV-2 is currently, and then, as more people became infected and therefore protected, these viruses could have become endemic and happy to cause infection where it could, among vulnerable people with weakened immune systems. “One of these now-common cold coronaviruses may have been responsible for an epidemic in the late 1800s that back then did not cause such mild disease,” says Nadia Roan, an associate investigator at the Gladstone Institutes, of the University of California, San Francisco. “But eventually as community immunity started to build, it became more endemic. It makes sense that—hopefully, potentially—Omicron could become one of the common coronaviruses when we as a community build up enough immunity against it.” Scenario #2: The virus could keep changing in unpredictable and possibly deadly waysBut a different, troubling scenario might also be possible. There is good evidence that suggests SARS-CoV-2 is an especially unpredictable virus—Omicron, after all, was an entirely new variant that shocked experts with its sudden and efficient ability to spread so quickly. In the fall of 2020, most virologists would have made an educated guess that if a new variant of SARS-CoV-2 were to emerge, it would be a souped up version of Delta—there was even talk of a Delta Plus. But Omicron surprised them all. “This isn’t a Delta-plus variant,” says Jeremy Farrar, president of the global health research foundation Wellcome Trust. “It’s from left field, and came out of a virus from 2020, which tells us something. We haven’t seen one lineage of this virus evolving into another lineage. We’ve seen things coming from a much broader spectrum. What that means is that we can’t expect the daughter or son of Omicron to then become the next thing we deal with. It could be something that comes from a different part of the virus’s evolutionary path.” What that suggests is that if we want to be prepared for future, potentially dangerous variants, we need to more closely monitor the virus around the world so we can identify any possibly highly transmissible variants earlier, and hopefully control them better. Read more: What We Learned About Genetic Sequencing During COVID-19 Could Revolutionize Public Health And as surprising as it was, Omicron probably didn’t appear overnight. SARS-CoV-2 likely evolved in stages, and the increasing transmissibility of what would become the Omicron variant went largely unnoticed. For example, about a year ago, researchers reported what should have been alarming changes to SARS-CoV-2 in three air passengers flying from Tanzania who tested positive for the virus when they landed in Angola. Those changes helped the virus evade the immune system better, and transmit more efficiently. Looking back, while their viral sequences did not quite match that of the variant we now know as Omicron, they showed enough worrying signs of adaptation to human immune defenses that we should have taken stronger action to contain those cases. 
“There is no reason to think that Omicron is the result of the virus mutating any faster,” says Luban. “It’s just that we never saw this version as it was developing, wherever that was.” That may have been in someone with a weakened immune system, who was only able to mount a partial defense against the virus, which was just enough selective pressure to push the virus to mutate, and continue mutating, until it hit upon the changes that helped it to become the efficiently spreading virus we now know as Omicron. Since the pandemic began, scientists have reported on cases of immunocompromised patients who have been able to harbor potentially mutating viruses for months or even a year. In other words, the next Omicron could already be out there, and we wouldn’t know it. Unless, that is, we dramatically improve our global surveillance efforts, and increase the amount of genetic sequencing of the virus that is done around the world. Laying bare the virus’s genome can provide the earliest hints of any changes, and clues as to which of these aberrations could be dangerous for human health. If we’d been able to identify the genetic changes that led to the Delta variant early on, for example, we could have prioritized locking down the parts of the world where those mutations were common, says Pardis Sabeti, professor at the center for systems biology at Harvard and member of the Broad Institute of Harvard and MIT. “That’s what genomic sequencing can do—stay ahead of diagnoses [of new cases] so we can try to develop countermeasures against something, including developing new therapies. It’s about ‘know thy enemy.’ If your enemy moves, you have to move.” With real-time genetic information, we could better know how to prioritize vaccine and treatment efforts. “The more information you have, the more thoughtful we can be in expending what are necessarily finite resources,” says Sabeti. Read more: Let’s Not Be Fatalistic About Omicron. We Know How to Fight It The problem, as Sabeti and Luban note, is that we don’t have such genomic eyes on the virus throughout the globe. Even in the U.S., where sequencing is becoming a priority, the Centers for Disease Control’s National SARS-CoV-2 Strain Surveillance program is sequencing only a small percentage of positive cases—in the single digits—each week. Only about five countries have sequenced double digit percentages of their positive cases so far. Experts’ best guesses at what comes nextHow likely is it that Omicron is indeed SARS-CoV-2’s last hurrah? Farrar puts the odds at 40% to 50%. One major reason the odds aren’t higher is that Omicron’s genetic changes make it more capable of evading capture by the antibodies the immune system makes, both after natural infection and vaccination. That helps the virus to spread more quickly—up to the tipping point at which if the virus is too good at spreading and causing disease, then it becomes self-defeating. “The virus doesn’t want to kill its host,” says Dr. Warner Green, former director of and current senior investigator at the Gladstone Institute of Virology and Immunology. “That’s counterproductive.” That could explain why Omicron is so impressively transmissible, but, for those with some protection, especially from vaccines, not particularly dangerous—making it possible that this particular version of the virus is the one that will persist in the human population for years and years to come. That’s the path public health experts hope SARS-CoV-2 will take, following the example of the other common coronaviruses. “The best scenario is for the virus to become so weakened it just becomes a vaccine itself,” says Greene. “It would spread but it wouldn’t cause severe disease. In that kind of setting, the virus would start to lose its foothold and become endemic in very small areas, replicating only when it finds people who are not previously infected or vaccinated.” That’s assuming, of course, that most of the world’s population is vaccinated, or recovered from being naturally infected with Omicron. The fewer opportunities SARS-CoV-2 has to replicate and produce more copies of itself, the fewer people will become infected, and the fewer people will get sick. Every variant in the virus’s short two-year history is the direct result of unchecked viral replication, so the surest way to turn COVID-19 from a pandemic into an endemic disease is to shut down as many of those opportunities as possible. “If we have learned anything from the past year, it is that variants will continue to emerge,” says Ho. “What will be helpful is to establish growing immunity, either from vaccines or infections. That will help protect the population from the next one.” from https://ift.tt/3u83jep Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
