|
When the opioid addiction crisis began to surge in the U.S. about a decade ago, Dr. Medhat Mikhael spent a lot of time talking to his patients about other ways to heal pain besides opioids, from other types of medications to alternative treatments. As a pain management specialist at MemorialCare Orange Coast Medical Center in Fountain Valley, Calif., he didn’t anticipate leaving behind the short-term use of opioids altogether, since they work so well for post-surgical pain. But he wanted to recommend a remedy that was safer and still effective. That turned out to be acupuncture. “Like any treatment, acupuncture doesn’t work for everyone, but the majority of my patients who have tried it have found relief,” he says. “When I started looking into studies, I discovered how much evidence there was behind this treatment, and that made me feel comfortable suggesting it as an alternative or a complement to pain medication and other treatments.” That blend of anecdotal success, research-backed results, and growing level of openness from the medical community are all driving the popularity of acupuncture as a therapy. According to a 2021 World Health Organization report, acupuncture is the most widely used traditional medicine practice globally, and it’s gaining traction in the U.S. In 2020, the Centers for Medicare & Medicaid services began covering acupuncture for the first time for chronic low back pain. Although scientists don’t yet understand all the nuances of how it works, research indicates it can have a significant effect on certain conditions, and it shows promise for others. What is acupuncture?The goal of acupuncture is the same now as it was thousands of years ago when it was first developed in China: restoring balance to the body, says Kevin Menard, a sports medicine acupuncturist and Traditional Chinese Medicine practitioner in Sag Harbor, New York. The practice is based on how energy, or qi, flows through the body along a series of channels called meridians—similar to the way nerves and vessels carry messages and blood throughout every system. “According to Chinese medicine theory, each meridian is related to a specific organ, and placing thin needles at certain points along these meridians can effect certain changes in the body to restore homeostasis,” says Menard. The needles aren’t the type you’d use to draw blood; they’re very thin and flexible, almost like bits of wire. Placement along the meridians is believed to cause reactions like sending more blood or lymphatic fluid to specific organs or allowing muscles to release in a way that reduces tension on joints and bones. The needles may also stimulate nerves and tweak nervous system regulation to result in a relaxation response, which relieves pain, Mikhael says. Acupuncture is also thought to stimulate the immune system and control inflammation, Menard says, two effects that can bring benefits throughout the body. Depending on the condition or injury, relief might happen with just one treatment, but it usually takes a series of sessions, Menard says, especially if an issue is complex or chronic. What the research saysResearch on acupuncture has been extensive, and so far, robust evidence supports its effectiveness for some, but not all, conditions. According to one analysis published in February 2022 in the BMJ that analyzed more than 2,000 scientific reviews of acupuncture therapies, the science is strongest behind acupuncture’s efficacy for post-stroke aphasia; neck, shoulder, and muscle pain; fibromyalgia pain; lactation issues after delivery; lower back pain; vascular dementia symptoms; and allergy symptoms. The National Institutes of Health (NIH) finds that acupuncture for pain relief tends to have the most evidence, especially for conditions that have become chronic like osteoarthritis and lower back pain, as well as tension headaches. A review of 11 clinical trials also suggests that acupuncture may help with symptoms associated with cancer treatment, the NIH notes. That’s been a booming area of interest for the field, says Sarah Weaver, an acupuncturist and massage therapist at Northwestern Health Sciences University in Minnesota, which focuses on integrative health professions, such as acupuncture, chiropractic, and Traditional Chinese Medicine. For cancer patients, sessions there can focus on reducing nausea, numbness, and tingling (called neuropathy), brain fog, low appetite, acute and chronic pain, and mood challenges that come with cancer care. “Often, people with cancer want to add complementary treatment that doesn’t affect their chemotherapy or radiation, and that’s where an option like acupuncture can be helpful,” she says. “It’s the reason more healthcare systems are bringing this treatment into their integrative care options.” What’s next in the fieldAcupuncture is far from a proven and accepted therapy for most conditions—even for the ones that show promise. That’s in part because the studies that support it are sometimes not high quality, and the field lacks standardized protocols that would better allow it to be scientifically evaluated, the recent WHO report finds. For instance, one 2016 research review analyzed studies looking at acupuncture for substance abuse and addiction. Among the 83 research articles included in the review, the researchers found substantial variations in study quality, acupuncture frequency, how long needles were left in the body during treatment, which points along the meridians were used, and other potentially important factors. That made it difficult to evaluate how effective the acupuncture really was. The field also lacks clear terminology and universally accepted agreement about the location of acupuncture points, researchers argue. Issues like these will have to be resolved to get more clarity, and to earn recommendations from reputable organizations in the future. International experts in the field are pushing to make clinical trials more rigorous in order to prove acupuncture’s utility for patient care and to help providers adopt the best practices as more benefits become clear. Some potential directions for future studies include studying how acupuncture may affect hormonal regulation, such as alleviating hot flashes in menopause or addressing menstrual irregularity. Research indicates that the practice can boost estrogen and other hormones, and acupuncture for gynecological issues is becoming more popular, says Menard. Some researchers are also focused on studying acupuncture’s impact on fertility; some small, preliminary studies indicate its use may be linked to getting pregnant sooner and having better outcomes from IVF treatments. Acupuncture for mental health issues like depression and anxiety is another major research direction, especially in terms of how these issues affect overall health. For example, chronic pain has often been linked to depressive symptoms, so researchers are looking at whether acupuncture can address both: a person’s pain and their depression. Researchers are hopeful. A study published in 2020 in the journal Frontiers in Neurology found that people with migraines who did acupuncture treatments had a lower risk of depression and anxiety, and tended to use medical services less often, compared to migraine patients who didn’t do acupuncture. As the evidence base expands, acupuncture will likely continue to grow in popularity. Although acupuncture has been used for centuries, only in the past decade has there been a seismic shift in acceptance by both Western medical doctors and patients, Menard says. Ongoing research efforts and increased interest from health systems means that the treatment may be part of more conversations like Mikhael had with his patients. “At the end of the day, doctors want their patients to feel better, and many people are looking for non-pharmaceutical paths for wellness,” Menard says. “Depending on the condition, those little needles can make a huge impact.” from https://ift.tt/vd0XMD6 Check out https://takiaisfobia.blogspot.com/
0 Comments
They were the words everyone has been waiting to hear—that the COVID-19 pandemic is dialing down from the five-alarm fire that flared up in 2020 to a somewhat lesser conflagration. On April 27, the U.S.’s chief medical advisor, Dr. Anthony Fauci, described the country as in a “transitional phase, from a deceleration of the numbers into hopefully a more controlled phase and endemicity” in an interview with the Washington Post. His comments come almost two years to the day after pharmaceutical manufacturers shipped the first batches of their COVID-19 vaccines for early testing. Fauci noted that those vaccines, as well as drug treatments that can control the virus in infected people, are largely responsible for the fact that the initial urgency of the pandemic as a public health threat is over. But COVID-19 itself isn’t quite finished with us. The virus continues to mutate, and the latest variations being reported out of South Africa—new subvariants of Omicron including BA.4 and BA.5—are sobering reminders that the virus isn’t standing still. “Pandemic” vs. “Endemic”Although we may be out of the urgent pandemic phase, we’re not quite ready to call COVID-19 endemic, which would mean the virus is still among us but relatively under control, similar to influenza. And it’s not clear when that will happen. And even if it does, health experts may not all agree about the transition. There are no hard and fast definitions for “pandemic” and “endemic,” and no thresholds for case numbers or deaths that mark a shift from one to the other. The World Health organization considers a pandemic to be an “epidemic occurring worldwide, or over a very wide area, crossing international boundaries and usually affecting a large number of people.” Experts have noted that these parameters say nothing about how quickly the outbreak is spreading, how much disease it’s causing, or what role immunity in the population plays. But those are the factors that are critical for public health experts and political leaders as they manage a pandemic. There are no metrics for determining when to dial down an initial urgent response, or to pull back on drastic measures such as lockdowns and mask mandates. That’s what the world is grappling with now—figuring out whether the risk of SARS-CoV-2 is now at a point where we can treat it more like influenza, by protecting ourselves as much as we can with immunization and basic hygiene such as washing our hands and covering our coughs, or whether we still need to manage SARS-CoV-2 as a serious enough threat for most people that we should maintain public health measures such as mask-wearing and social distancing. Read more: Most Americans Have Had COVID-19. That Doesn’t Mean They Won’t Get It Again What a “controlled pandemic” looks likeFauci argues that we are somewhere in between those two situations, describing our current status as a “controlled pandemic”—not quite the urgent threat of a pandemic, but again not quite ready for the ease of mind that comes with being in an endemic phase of an outbreak. And the numbers support that: Since the beginning of the year, cases in the U.S. have dropped dramatically, from an average of 700,000 to 800,000 a week to 30,000 to 50,000 a week. About 66% of the U.S. population is now fully vaccinated against COVID-19, and deaths from the disease have declined steadily since January. We are clearly not in the same vulnerable place we were in 2020. The vaccines have provided some barrier to the virus, and that counts for a lot. But that immunity still isn’t enough to declare COVID-19 over. Nevertheless, those numbers encouraged a push to loosen public health restrictions that have been in place since 2021—federal mandates that people wear masks in indoor settings, and on public transportation including subways, buses, trains and planes, as well as requiring proof of vaccination for certain gatherings at sports and entertainment complexes. In April, a U.S. District judge in Florida struck down the federal mask mandate, declaring that it was unlawful and that the Centers for Disease Control had overstepped its authority in imposing it. The Biden Administration is appealing the ruling, but in the meantime, airlines and most public transit systems no longer require passengers to wear masks. That coincided with an uptick in cases of COVID-19—there’s no direct way to prove one caused the other, but the coincidence is hard to ignore. After remaining at about 24,000 to 25,000 new infections a week in early April, cases started to inch upward again at the end of the month to nearly 50,000 a week on average. Hospitalizations are also creeping upward, although those trends lag behind case rates. Steps towards a truly endemic COVID-19 virusThose trends suggest that it may be too early to relax our vigilance over COVID-19, which remains a potent threat for a number of reasons. First, no vaccine is 100% effective in protecting against infection or disease, and the COVID-19 shots are no exception. While highly effective in warding off the worst COVID-19 symptoms from the original virus strain emerging from China, the shots are less effective in protecting against newer variants of SARS-CoV-2. And the virus continues to mutate, with each version appearing to improve on the last strain’s ability to infect quickly and efficiently. Fortunately these changes haven’t led to a more virulent strain so far, but they could veer in that direction, and cause more serious disease on top of being more transmissible. If that happens, the vaccines and drug treatments currently available might provide little, if any, protection at all. That leads to the second reason that COVID-19 isn’t fading into the background any time soon. Despite the effectiveness of the vaccines, scientists still don’t know exactly what it takes to fully protect someone from COVID-19. That question actually breaks down into two related queries: What does it take to prevent infection in the first place, and what level of immunity is needed to protect against serious illness? Even into the third year of the COVID-19 pandemic, scientists still don’t have solid answers for either. Read more: Many Americans Are Celebrating the End of COVID-19. Here’s What It Feels Like When You’re Not While the mRNA shots in particular are effective at curbing COVID-19 disease, reducing the rates of COVID-19 symptoms by more than 90% among people who were immunized, the vaccines have been less effective in protecting people from getting infected in the first place. That’s not unusual for a vaccine, since the best way to block infection is with a pre-existing store of antibodies that can stick to the virus and interrupt them from infecting cells—and before getting immunized, most people in the world didn’t have any antibodies against SARS-CoV-2. And even after getting vaccinated, antibody levels drop after a few months, which is why health officials have recommended booster doses. Those boosters have been slightly better at reducing risk of infection for this reason, but the vaccines are still not designed as a powerful way to stop infection. They are far better at preventing serious COVID-19 disease. But even there, it’s still not clear exactly how much of an immune response, or what type, is enough to stop severe COVID-19 symptoms that can lead to hospitalization and even death. Studies of people who have been vaccinated, as well those involving people who have been naturally infected with SARS-CoV-2, are trying to shed some light on this, but scientists still can’t point to exactly what kind of immune reaction will be essential to finally push SARS-CoV-2 back. Such knowledge about what scientists call the correlates of immunity could go a long way toward shaping U.S. policy on booster shots in the fall. For now, the Food and Drug Administration and other public health experts are relying on antibody level data as a proxy to gauge how well vaccines work and what type of immunity is needed. But in a recent meeting of the FDA’s vaccine advisory committee, the experts raised concerns about how reliable the current metrics of antibody levels are in serving as surrogates for these correlates of immunity. Until further research reveals how much immune protection is enough, it’s not likely that the world will move past seeing COVID-19 as a continuing pandemic threat, albeit, as Fauci proposed, one that is under better control now than when it first emerged in 2020. That’s why the White House, with the support of the CDC, is pushing back on lifting the federal mandate for mask-wearing on public transit, and stressing that while the hospitalization and death numbers are trending in the right direction, the virus is far from gone and is still a threat to public health. It’s not likely that there will be consensus any time soon on when the pandemic shifts from even Fauci’s so-called “controlled” phase into becoming endemic. In the meantime, rather than waiting on broad declarations on whether the pandemic is over, some health experts are urging people to start making their own informed decisions about which behaviors and situations feel safe to them. If they have underlying chronic conditions that can put them at higher risk of severe COVID-19, such as diabetes or asthma, for example, or if they have compromised immune systems, it makes sense for them to continue wearing masks even on planes and trains where they aren’t required. Or if people live in households with elderly people or with children under six years old who aren’t eligible to get vaccinated yet, then continuing to wear masks in certain indoor settings and avoiding crowded situations might be wise. Government and global health organization statements about the pandemic are critical for helping nations to navigate responses and allocate resources for addressing public health, but once those tools are in place, it’s up to us as individuals to use them in the combination and frequency that provides us with the most protection in our specific circumstances. Even if SARS-CoV-2 becomes endemic like the flu, it will remain a threat for certain groups, just as influenza does. For those people, it will be important to maintain all the behaviors that protect them from infection. For those who are less vulnerable, easing some of those protection measures might make more sense. While mandates have served as guides for the best way to battle the pandemic, going forward it will likely fall increasingly on individuals to rely on those guides to forge their own path forward as each of us learns to live with COVID-19, in whatever form it takes. from https://ift.tt/h7Dpx2g Check out https://takiaisfobia.blogspot.com/ Black and Hispanic Americans remain far more cautious in their approach to COVID-19 than white Americans, recent polls show, reflecting diverging preferences on how to deal with the pandemic as federal, state and local restrictions fall by the wayside. Despite majority favorability among U.S. adults overall for measures like mask mandates, public health experts said divided opinions among racial groups reflect not only the unequal impact of the pandemic on people of color but also apathy among some white Americans. Black Americans (63%) and Hispanic Americans (68%) continue to be more likely than white Americans (45%) to say they are at least somewhat worried about themselves or a family member being infected with COVID-19, according to an April poll from The Associated Press-NORC Center for Public Affairs Research. Throughout the pandemic, Black and Hispanic communities have experienced higher rates of illness and death from COVID, said Amelia Burke-Garcia, public health program area director at NORC. Those experiences have resulted in greater levels of stress, anxiety and awareness of the risks of catching COVID-19, she said, which means people of color are more likely to feel measures like mask mandates are needed. Read More: Most Americans Have Had COVID-19. That Doesn’t Mean They Won’t Get It Again “We’ve seen these trends endure throughout the entire pandemic,” Burke-Garcia said. “What we’re seeing now as mitigation measures are being rolled back is there’s still great concern amongst Black Americans and Hispanic Americans around the risk of getting sick.” 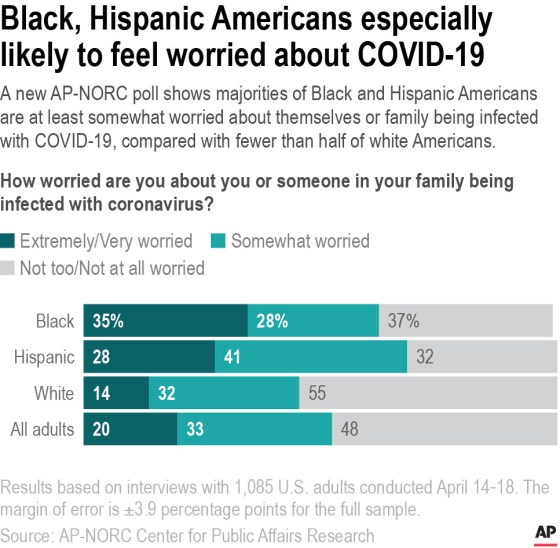
Seventy-one percent of Black Americans say they favor requiring face masks for people traveling on airplanes, trains and other types of public transportation. That’s more than the 52% of white Americans who support mask mandates for travelers; 29% of white Americans are opposed. Among Hispanic Americans, 59% are in favor and 20% are opposed. The poll was conducted before a ruling by a federal judge scuttled the government’s mask mandate for travelers. In Indiana, Tuwanna Plant said she sees fewer and fewer people wearing masks in public, even though she said she has been diligent in always wearing one. Plant, who is Black, said she sees people treating the pandemic like it’s over, and she wants the mask mandate to continue. Plant, a 46-year-old sous chef, said she had some concerns about getting the vaccine and took every other precaution, such as cleaning and masking, to avoid getting sick but recently was hospitalized for COVID-19. The experience scared her — she has a preexisting lung condition, and knew family members who died from COVID-19. She said she plans to get vaccinated as soon as she can. “I called my children while I was in the emergency room,” Plant said. “I didn’t know … if it was going to get better or worse, I didn’t know. So it was the experience for me altogether.” Dr. Celine Gounder, an infectious disease specialist and epidemiologist and editor-at-large at Kaiser Health News, said people’s lived experiences deeply shape how they perceive the pandemic. Anecdotes and personal experience can have a larger impact on behavior than numbers, she said, and people of color are more likely to have had negative experiences with health care prior to and during the pandemic. While new medicines and vaccines have made it easier to treat COVID-19, Gounder said many people still face systemic barriers to accessing that medical care. Others risk losing their jobs or are unable to take time off if they do fall ill, she said, or cannot avoid things like public transit to reduce their exposures. “When people argue that they don’t have to mask on the plane, that means something very different for someone who has access to all of these new innovations than it does for somebody who has no health insurance, who struggles to care for an elderly parent and their children, who’s maybe a single mom working in a job where she has no paid sick and family medical leave,” Gounder said. “It’s just a completely different calculation.” Read More: As COVID-Era Restrictions End, Disabled Americans Want to Avoid a ‘Return to Normal’ In January, an AP-NORC poll showed Black and Hispanic Americans were more likely than white Americans to feel certain things would be essential for getting back to life without feeling at risk of infection. For example, 76% of Black Americans and 55% of Hispanic Americans said it was essential for getting back to normal that most people regularly wear face masks in public indoor places, compared with 38% of white Americans. Last month, an AP-NORC poll showed Black and Hispanic Americans, 69% and 49%, were more likely than white Americans, 35%, to say they always or often wear a face mask around others. Lower support for mask mandates and other precautions among white Americans may also reflect less sensitivity towards what occurs in communities of color. In a 2021 study of mask wearing during the early part of the pandemic, researchers found that mask wearing among white people increased when white people were dying at greater rates in the surrounding community. When Black and Hispanic people were dying, mask usage was lower. Berkeley Franz, a co-author of the paper, said that in addition to residential segregation that separates white people from communities of color, past research has shown that white people can display ambivalence toward policies that they believe mostly help people of color. “Anti-Blackness is really pervasive and has tremendous consequences, both in terms of the policies that get passed, and what doesn’t,” Franz said. “White people can still have really racist actions without seeing themselves that way and understanding the consequences. It’s largely below the surface and unintentional but has tremendous consequences in terms of equity.” Communities of color also have a different perception of risk from the pandemic than their white counterparts, said Michael Niño, a sociology professor at the University of Arkansas who co-authored a paper on race, gender and masking in the pandemic. “Masking is something that is relatively cheap, it’s effective, and it’s something that can be easily done,” he said. “It doesn’t require any sort of governmental response. These broader histories of racism and sexism in the United States are most certainly shaping some of the patterns we’re seeing.” ___ The AP-NORC poll of 1,085 adults was conducted April 14-18 using a sample drawn from NORC’s probability-based AmeriSpeak Panel, which is designed to be representative of the U.S. population. The margin of sampling error for all respondents is plus or minus 3.9 percentage points. from https://ift.tt/FopOecZ Check out https://takiaisfobia.blogspot.com/ Odds are, you’ve had COVID-19—whether you know it or not. Almost 60% of people in the U.S. have antibodies in their blood that suggest they’ve been infected by SARS-CoV-2, the virus that causes COVID-19, according to new estimates from the U.S. Centers for Disease Control and Prevention. But that doesn’t mean 60% of people in the U.S. are immune to COVID-19. “We know that is not what this means. Reinfection happens,” said Dr. Kristie Clarke, co-lead for the CDC’s COVID-19 Epidemiology and Surveillance Taskforce Seroprevalence Team, during a press briefing on April 26. “Protection from vaccination and protection from previous infections does wane over time.” Even two years and millions of infections into the pandemic, researchers are still learning about immunity to the virus, and how long you can expect to remain disease-free after a shot or illness. Here’s what the latest science says about immunity to COVID-19. If I already had COVID-19, will I get it again?Your immune system mounts a few different defenses against SARS-CoV-2. White blood cells called B cells produce antibody proteins, which help fight off the invader. Meanwhile, T cells, another type of white blood cell, can kill off cells that have been taken over by the virus. A study from U.K. researchers published in the New England Journal of Medicine in March found that infection-related immunity stays strong for up to a year, then began to wane—whereas the protection offered by two doses of a Pfizer-BioNTech vaccine begins to wane at around six months. Meanwhile, a research review published in the Annals of Internal Medicine in April concluded that people who’d recovered from COVID-19 had significant protection against reinfection for at least seven months. But all of that research was done before the emergence of the Omicron variant, which is more contagious than previous strains. “We can’t really predict how the protection will work for the next variant or over a period of time,” says co-author Dr. Mark Helfand, a professor of medicine at the Oregon Health & Science University. Children may hold onto their antibodies even longer than adults, according to a new study from researchers at the Indiana University School of Medicine. Six months post-infection, more kids than adults still had antibodies capable of neutralizing the virus, they found. While those findings should bring some comfort to people who have had COVID-19, there are no guarantees when it comes to immunity. (A woman in Spain recently made headlines for testing positive for COVID-19 twice, only 20 days apart.) Some people develop more antibodies after an infection than others. It’s also not clear exactly how antibody levels correlate with protection against infection, so a positive antibody test doesn’t necessarily mean you’re immune to the virus, Clarke said during the CDC briefing. Dr. Bruce Farber, chief of infectious diseases at Northwell Health in New York, says there’s no way to say for sure how long someone who has recently recovered from COVID-19 can stop worrying about being reinfected. But, he allows, it would be “very unusual” to get COVID-19 within 90 days of a previous case. If I’m fully vaccinated, am I immune to COVID-19?COVID-19 vaccines also prompt the body to produce antibodies and trigger a T-cell response, though they’re different from those the body produces naturally. Vaccines provide strong and durable protection against severe disease and death, but their effectiveness against infection wanes over time, so your risk of getting sick is lowest shortly after your most recent dose. A research review published in the Lancet in March analyzed data from prior studies that assessed the effectiveness of different COVID-19 vaccines, including those made by Moderna, Pfizer-BioNTech, AstraZeneca, and Johnson & Johnson. Across brands, vaccines’ ability to prevent symptomatic disease dropped by 20% to 30% after six months, even though they remained good at preventing severe disease and death, the researchers found. This review was also published before the Omicron variant--against which vaccines are less effective—began spreading widely. Even with Omicron circulating, however, someone who’d been vaccinated was 2.4 times less likely to test positive for the virus in March than an unvaccinated person, according to the CDC. Anyone who is unvaccinated, whether they’ve had COVID-19 or not, should still get their shots, says Dr. Jessica Ridgway, an associate professor of medicine at the University of Chicago who co-authored a recent study on COVID-19 reinfection. “They’re incredibly safe and having that additional level of immunity would definitely be helpful for preventing COVID,” she says. Further, research shows that getting a booster dose can help bring protection to even higher levels. What if I’m vaccinated and had COVID-19?If you’ve recovered from COVID-19 and gotten a COVID-19 vaccine, you have what’s known as “hybrid immunity.” Studies suggest this type of protection is better than either vaccination or exposure alone, because you benefit from both natural and vaccine-derived defenses. “The best immunity, no question in my mind, is hybrid immunity,” Farber says. Of course, you should never try to catch COVID-19 for the sake of gaining hybrid immunity. While it’s very unusual for someone who is vaccinated and generally healthy to have a severe case of COVID-19, complications can happen. People have gotten Long COVID even when they’re fully vaccinated and experience few symptoms, for example. Will I need to keep getting COVID-19 boosters forever?The U.S. Food and Drug Administration (FDA) recently authorized a second round of boosters for people ages 50 and older, as well as some immunocompromised people across age groups. Additional boosters haven’t yet been authorized for the entire population—but there’s been lots of speculation about whether they will be, since vaccine-related immunity wanes with time. The FDA’s vaccine advisory committee met in April to discuss ways to streamline and improve booster strategy moving forward. An annual dose, as with flu shots, is a possibility—but the SARS-CoV-2 virus mutates in less predictable ways than the influenza virus, so it’s challenging to make in advance a booster that would target whatever strain is circulating later on. A better model could be developing boosters that provide immunity to multiple variants. That science is underway now, but it’s too soon to say exactly what future boosting strategies will look like. from https://ift.tt/KVNt3dM Check out https://takiaisfobia.blogspot.com/ Infant-formula makers use social media and influencers to target women and boost sales, undermining efforts to increase breastfeeding rates, according to a new study by the World Health Organization. Companies use personalized content through apps, paid influencers and advice forums to reach consumers, the WHO report said, adding these are often not recognizable as advertising. The results build on the WHO’s largest ever study on infant formula marketing, and come at a challenging time for infant-formula makers. The pandemic has led to lower birth rates just as competition from local rivals has become more intense in key market China. Nestle SA, for example, has been trying to revive the business in that market, while Reckitt Benckiser Group Plc has started a sale of its baby nutrition business after exiting China last year. The report analyzed 4 million social media posts about infant feeding published in the six months through June last year. The posts reached almost 2.5 billion people, according to the report. It found that firms selling formula uploaded content around 90 times per day, reaching 229 million users — three times as many people as are reached by informational posts about breastfeeding from non-commercial accounts. 
“This pervasive marketing is increasing purchases of breast-milk substitutes and therefore dissuading mothers from breastfeeding exclusively,” the report said. The marketing practices of infant-formula companies vary widely, Marie Chantal Messier, Nestle’s head of food and industry affairs, said following the publication of WHO’s initial report in February. The Swiss company doesn’t promote formula for babies up to 12 months in 163 countries, and will voluntarily stop promoting formula for infants up to six months around the globe by the end of the year, she said. “Danone encourages maternal breastfeeding and even encourages the WHO recommendations, as one of the first companies to also stop advertising products from 0 to six months,” CEO Antoine de Saint-Affrique said at the company’s AGM earlier this week. He said Danone is “extremely responsible in its approach.” from https://ift.tt/XyBRrgK Check out https://takiaisfobia.blogspot.com/ Back in 1982, when I first began my career as a family practitioner in a small town of Boston, I was confident that the care I’d provide would be as effective as the care patients receive anywhere in the world. At the time, the death rate for Americans was lower than that of comparable countries, resulting in 128,000 fewer deaths annually. Although healthcare was expensive—costing 2.3% more of our GDP than the average of 11 other wealthy countries—the rapid growth of HMOs and managed care plans promised to make our healthcare even more effective and efficient. Over the ensuing four decades, however, the opposite has occurred. The same age-adjusted mortality rate has improved so much more in comparable countries that, by 2017, an excess 478,000 Americans were dying each year. This translates into an extra 1,300 deaths daily, equivalent to three jumbo jets crashing every day. The everyday poor health of Americans and the inability of our healthcare system to mitigate preventable deaths amounts to a crisis that dwarfs even the COVID-19 pandemic. And our excess spending has risen to 6.8 percent of GDP, or $1.5 trillion per year. [time-brightcove not-tgx=”true”] This raises a key question: Why have so many smart, well-trained doctors stood by as American healthcare descended into a state of profound dysfunction? The answer lies in the gradual, nearly invisible commercial takeover of the medical “knowledge” that doctors are trained to trust. This transition started in the 1970s, when the acceptance rate of grant applications for funding from the National Institutes of Health shrank—from roughly half of medical research applications to one-third. Then, in 1981, President Ronald Reagan slashed government support of university-based medical research, further pushing academic researchers into the waiting arms of industry, especially pharmaceutical companies. Following the 1980 passage of the University and Small Business Patent Procedures Act, nonprofit institutions and their researchers were allowed to benefit financially from the discoveries made while conducting federally funded research. Former president of Harvard University Derek Bok expressed concern about the growth of commercial activities within academia: “Making money in the world of commerce often comes with a Faustian bargain in which universities have to compromise their basic values—and thereby risk their very souls…” The biggest shift was, however, still to come. Over the past few decades, the drug companies have taken over most of our clinical research. In 1991, academic medical centers (AMCs)—hospitals that train doctors and conduct medical research—received 80 percent of the money that industry was spending to fund clinical trials. The drug companies relied on academic researchers for their expertise in designing studies, enrolling patients, and analyzing the data. This arrangement allowed academics to receive the funding they needed while still preserving much of their independence. But by 2004, the percentage of commercially funded clinical trials conducted by AMCs had fallen from 80 to just 26 percent. A look at the research contracts between corporations (mostly Big Pharma companies) and academic medical centers shows that 80% allowed the commercial funder to own, and thus control, the data from jointly conducted research. Furthermore, fully half of the research contracts between drug companies and academic institutions—the partnerships with the highest likelihood of upholding rigorous research standards—allowed industry insiders to ghostwrite clinical trial reports for publication in scientific journals, relegating the named authors to the position of “suggesting” revisions. Nonetheless thorough peer review ensures that these reports are accurate, right? Wrong. Unbeknownst to almost all doctors, peer reviewers are not granted access to the underlying data that serves as the basis for the reported findings. The drug companies own that data and keep it confidential as “corporate property.” Reviewers must rely on brief data summaries included in the submitted manuscripts. Peer reviewers at even the most prestigious medical journals cannot possibly attest to the accuracy and completeness of the articles they review. This sham was exposed in 2005 when the editors of an article published in the New England Journal of Medicine admitted they had not seen relevant data from a clinical trial involving Merck’s arthritis drug Vioxx. Five years earlier, the article had extolled the drug’s safety even though neither the editors nor the peer reviewers had been granted access to underlying data, which showed three heart attacks that had occurred in patients treated with Vioxx were not reported. Had this data had been properly disclosed and analyzed when the manuscript was first submitted, the article would have shown that Vioxx significantly increased the risk of heart attack five-fold when compared to over-the-counter naproxen (Aleve). And many of the estimated 30,000 Americans who died as a result of taking Vioxx after the incomplete article was published would not have been exposed to the drug. To this day, Big Pharma companies remain unwilling to disclose their underlying clinical trial data. The most recent example involved Pfizer’s COVID-19 vaccine. In September 2021, one month after the vaccine had been granted full approval by the U.S. Food and Drug Administration (FDA), a group of medical researchers and scientists sued the agency for the release of 451,000 pages of scientific documents it had evaluated prior to granting the vaccine full approval. Even though the agency required only 108 days to sufficiently evaluate these documents before granting the vaccine formal approval, the FDA (with Pfizer wanting to join the lawsuit), argued that the fastest they could release the data was five hundred pages per month, meaning that it would take seventy-five years before the documents were released in full. On January 6, 2022, U.S. District Judge Mark Pittman ruled that the FDA must release 55,000 (not 500) pages of the documents each month until complete. I want to be clear that I’m a strong advocate of getting vaccinated and boosted (especially for people age 65 and older), the CDC’s analysis of real-world data shows that last December unvaccinated adults had 41 times the risk of dying of COVID-19 compared to fully vaccinated and boosted adults. But I believe just as strongly that doctors and the public must have access to the underlying clinical trial data that the FDA approval is based upon now—not in seventy-five years. The lack of transparency of clinical trial data in peer review is similar around the world. But the effect is far greater in the U.S. because of our unique pharmaceutical policy. We have no formal assessment that compares the medical benefit and economic value of new drugs to older therapies, so health-care professionals do not have access to this critically important information. Federally funded clinical practice guidelines are not allowed to include the relative cost of therapies in their recommendations, which means there is no consideration given to the chance that a drug may unnecessarily bankrupt patients or inflate the cost of health insurance. Further, the price of brand-name drugs is unregulated in this country, which is why they cost 3.5 times more in the U.S. than in other OECD countries. And unregulated prices increase the reward-to-risk ratio for overly aggressive marketing practices in the U.S. The industry’s control over what doctors believe about optimal therapeutics explains why new, expensive drugs are used more liberally in the U.S. than other countries. Without access to the actual clinical trial data, medical journals are publishing unvetted articles that doctors then rely on to treat their patients. Although prescription drugs “only” account for 17% of U.S. health-care expenditures, this has become a “tail wags dog” situation: The drug companies control the “knowledge” that informs doctors’ clinical decisions. This leads to soaring pharmaceutical profits and crippling healthcare costs, while doctors have no way of knowing which therapies are more effective—or more efficient. Americans deserve better. from https://ift.tt/oZpICNy Check out https://takiaisfobia.blogspot.com/ When you think about hypnosis, what do you visualize? For many, it’s a clock-swinging magician or a comedy act that forces an unwitting volunteer to make embarrassing public admissions on stage. But hypnosis has a surprisingly robust scientific framework. Clinical research has shown that it can help relieve pain and anxiety and aid smoking cessation, weight loss, and sleep. It can help children and adolescents better regulate their feelings and behaviors. Some people can even use “self-hypnosis” to manage stress, cope with life’s challenges, and improve their physical and emotional health. Hypnosis creates “a non-judgmental immersive experience,” says Dr. David Spiegel, a Stanford University psychiatrist and leading researcher of hypnosis. It’s been used in various forms for centuries, but it wasn’t until 1843 that the Scottish surgeon Dr. James Braid popularized the term “hypnosis.” Braid’s central discovery—that concentration can guide the brain toward a more suggestible state—was and remains controversial. But physicians have continued to test and teach the technique over the centuries with great success, Spiegel says. Today, a psychologist, psychiatrist, or other healthcare professional certified in hypnotherapy will first screen a potential client for their ability to be hypnotized using a validated suggestibility scale. (Not everyone is equally susceptible to hypnosis, but research has found that about two-thirds of adults are.) The hypnotherapist will talk with them about what sort of sensory experiences make them feel safe, like a lakeshore retreat or a beach vacation. Then, the hypnotherapist will conjure that imagery—focusing, for example, on the salt spray of the ocean, seagulls calling overhead, and sun-kissed skin—to help the person go deeper into the calming visualization. If done right, the patient’s physical surroundings will melt away. The result is a powerful combination of dissociation, immersion, and openness to new experiences, which culminates in what was once called a “trance,” but which modern hypnotherapists simply refer to as a “hypnotic state.” It can be achieved in just a few minutes, Spiegel says. Such scene-setting techniques can create the ideal stage for positive transformation, says Binghamton University psychology professor Steven Jay Lynn. During hypnosis, people are more open to the suggestions of the hypnotherapist, whether those ask the patient to detach themselves from a past painful experience or visualize a solution to their problem. For some people, these changes may be catalyzed in a one- or two-hour session. For others, hypnotherapy or self-hypnosis may be a regular part of their mental health care. “Hypnosis can modify consciousness in many ways,” Lynn says. This state of deep relaxation isn’t particularly difficult for most people to dive into or emerge from. It’s similar to a “flow state,” Spiegel says, or an altered state of consciousness in which a person is so immersed in a given activity, their focus narrows and their sense of time shifts. It’s also reminiscent of what happens during meditation, except instead of training people to tune into the present moment, hypnosis makes them more receptive to suggestion. Like meditation practice, many people are capable of doing hypnosis on their own, Spiegel says. In 2020, he co-founded Reveri, a subscription-based self-hypnosis app that’s structured a lot like Calm or Headspace. A user can access recordings that guide them into a hypnotized state, after which they’re given suggestions or statements that lead them toward a goal the person selects before the session. “We do it all the time,” Spiegel says of entering and exiting these mental states, “but in hypnosis you do it more.” Brain-imaging studies have helped to illuminate what happens inside the hypnotized brain, though much still remains a mystery. During hypnosis, activity in a brain region that helps people switch between tasks quiets down, Spiegel says. This same region seems to disconnect from another area responsible for self-reflection and daydreaming—which may be why hypnotized people aren’t worried about who they are or what they’re doing. Researchers have also found that hypnosis can calm brain regions that help control autonomic functions like heart rate, blood flow, and breathing. This is likely what leads to the physical relaxation that’s a hallmark of hypnosis, Spiegel says. One of the most interesting modern applications of hypnosis is in the operating room, says Lorenzo Cohen, director of the Integrative Medicine Program at the University of Texas MD Anderson Cancer Center. For some localized breast cancer surgeries, namely lumpectomies, the center lets patients choose between general anesthesia or a localized anesthetic and hypnotherapy. Those who choose the second option remain fully awake during their surgery, but a hypnotherapist first helps them enter a state of deep relaxation, or “hypnosedation,” Cohen says. “The local [anesthesia] should be doing its thing,” Cohen says. “The rest is in your head.” More than 30 clinical trials have affirmed the use of hypnosedation, says Cohen (who is also researching the practice). Studies have shown that people who received hypnosedation experienced less preoperative anxiety, required less pain medication during surgery, and reported less post-operative pain intensity, nausea, fatigue, and discomfort than people who chose general anesthesia, Cohen says. “The hypothesis is that the patients who are under general anesthesia, even though they’re not conscious, are having an intense stress response,” he says. This can suppress an immune system that, in cancer patients, is already compromised by the disease and its treatments. When patients choose hypnosis, Cohen believes the body’s fight-or-flight response may be reduced. Despite the mounting evidence, hypnosis is not without skeptics. Randomized controlled trials have found that hypnosis can help with pain and anxiety associated with a range of medical conditions, but even the best studies can’t meet the gold-standard of a double-blind design, Spiegel says. While patients and practitioners can be kept in the dark about what pill they’re administering or receiving, it’s almost impossible to design a study where neither side knows hypnosis is being delivered, he adds. And historically, the power of hypnosis hasn’t always been wielded responsibly. The imaginative potential of hypnosis has been shown to create false memories—sometimes with devastating effects. At least 27 states ban hypnotically-elicited testimony from appearing in court. Hypnotherapists should avoid using the technique to “recover” memories, Lynn says. But when conducted by a trained professional and properly applied, modern hypnotherapy can provide powerful results. Susceptibility to suggestion is often “viewed as a liability or a weakness,” Spiegel says, “but it’s really a strength.” from https://ift.tt/njRiBYI Check out https://takiaisfobia.blogspot.com/ On April 28, Moderna submitted a request to the U.S. Food and Drug Administration (FDA) for emergency use authorization for its COVID-19 vaccine in children between six months and six years old. The Cambridge, Mass.-based company is now the second to request permission for an mRNA vaccine against COVID-19 for use in that age group. Pfizer-BioNTech, the other mRNA vaccine maker, requested the same authorization for its shot in February, under a rolling submission process in which the company would provide additional data for the agency to review. The FDA initially planned to review Pfizer-BioNTech’s request at that time, but decided to postpone a scheduled meeting of its independent panel of experts until the company provided additional data. The studies on younger kids, completed in December 2021, showed underwhelming protection in children two to four years old, although the vaccine did generate good immunity among those six months to two years old, and the company has since tested an additional, third dose of the vaccine to produce a stronger immune response. The FDA will likely compare those data from Pfizer-BioNTech against those from Moderna in these youngest children, which are now available. Moderna’s recent studies show that vaccinated children from six months to six years old were able to generate antibodies that could neutralize SARS-CoV-2 at levels similar to those produced in vaccinated adults. One difference: the children in Moderna’s study were given a quarter of the dose given to adults—which still produced a robust immune response, which could be due to the fact that children’s still-developing immune systems might respond more aggressively to vaccines. That’s a positive, since lower doses have been linked to fewer side effects. As with the Pfizer-BioNTech shot, Moderna’s study also found that antibody levels were higher among the youngest children, from six months to two years old, compared to levels among two to six year olds. Researchers aren’t clear why the youngest kids generated stronger immune responses, but it may be related to their faster growing bodies, including the organs that are responsible for making antibodies and can contribute to a more active response. “We learned that you can give the Moderna vaccine to little kids and it’s safe and effective,” says Paul Burton, chief medical officer at the company. “As a dad and as a physician, that’s really important. Little kids can mount a very robust immune response when vaccinated against the COVID-19 spike protein, which says to me that we can safely protect them. That’s good news for kids and good news for their caregivers.” Moderna’s team tested its vaccine in this group against the Omicron variant, which is now responsible for the bulk of new infections. The efficacy in protecting kids from six months to six years old from an Omicron infection ranged from 37% to 51%, depending on the children’s ages, with the youngest enjoying stronger efficacy. While that’s lower than the initial vaccine efficacy seen against the original strain of the virus, which was above 90%, the 40-50% range is similar to that seen among adults who were immunized with Moderna’s shot and exposed to Omicron. Moderna’s scientists are already studying a booster dose for childern over six (for whom the vaccine is already authorized), and also plan to start investigating whether a booster might be necessary for children six months to six years. Burton expects those data will be available before the end of the year. The FDA will now review the company’s data and make a decision about whether Moderna’s vaccine is safe and effective enough for the youngest children; the agency has not scheduled a meeting of its panel of independent experts yet. from https://ift.tt/2eAr4xp Check out https://takiaisfobia.blogspot.com/ From multivitamins and melatonin to fiber and fish oil, Americans who are trying to boost their health and immunity have a plethora of supplements to choose from. An estimated 58% of U.S. adults ages 20 and over take dietary supplements, according to the U.S. Centers for Disease Control and Prevention, and the supplement industry is valued at more than $30 billion a year. Supplement use has been growing rapidly over the past few decades along with the wellness industry. “The popular belief is that a supplement is going to be helpful for promoting health,” says Fang Fang Zhang, a professor at Tufts University’s Friedman School of Nutrition Science and Policy. She has found that people who use supplements more frequently are also more likely to have a higher level of education and income, a healthier lifestyle, and a greater likelihood to eat a healthy diet and exercise. “So those who are taking supplements are more health-conscious overall,” she says. But if you’re already healthy, most supplements may not do much to improve your health or stave off death. “There’s no clear evidence to suggest benefits of dietary supplement use for many popular or common health outcomes,” says Zhang. In some cases, supplement use could even be harmful. A 2015 study published in the New England Journal of Medicine found that there are an estimated 23,000 emergency department visits every year in the U.S. for adverse events related to the use of dietary supplements, many involving cardiovascular issues from weight-loss or energy products. “Particularly when we use very high dose implementations, sometimes we might be doing more harm than good,” says Eliseo Guallar, professor of epidemiology and medicine at Johns Hopkins Bloomberg School of Public Health. Some experts have called for more stringent federal regulation to ensure that supplements are safe and effective. Until then, consumers may want to proceed with caution and do their due diligence before taking supplements. What are supplements good for?Vitamins, minerals, and many other micronutrients are vital to the body’s functioning and are a crucial part of a good diet. But eating nutrients in food is not the same as taking them in supplement form. “Dietary supplement use is not a substitute for a healthy, balanced diet,” says Zhang. Vitamin and mineral supplements can be extremely useful when prescribed for people with nutritional deficiencies and certain illnesses. “High-quality supplements should be widely available, and we need them as part of medical treatment,” says Dr. Pieter Cohen, an associate professor at Harvard Medical School and an internist at Cambridge Health Alliance. However, much packaged food in the U.S. is already fortified with additional nutrients, making nutritional deficiencies uncommon in the general population. For most people, supplements may offer questionable benefit. In an analysis published in 2020 in the BMJ, Zhang reviewed results from several trials and found no clear evidence that nutritional supplements like vitamins and minerals are helpful in healthy people for preventing chronic diseases such as cardiovascular disease or cancer. The evidence is even more muddled for certain plant-derived dietary supplements known as botanicals, such as echinacea and ginkgo. Scientists have tried to decipher the effects of many botanicals or nutritional supplements, but the field is still littered with weak or contradictory results. “We know a lot,” says Guallar. “The problem is that sometimes the claims go beyond what we know.” Many of the health claims that companies slap on their supplement labels may extrapolate results seen in animals to humans or make too much of what are still preliminary findings. “These products should not be promoted as if they will have benefits for our health when it’s never been proven that they work in humans,” says Cohen. As a result, consumers may not know what to make of supplement claims and may be confused about which supplements are useful. “This is also combined with commercial pressure to promote some of these supplements,” says Guallar. How dietary supplements are promoted and advertised is itself a function of how they’re regulated by the U.S. Food and Drug Administration (FDA). Regulated as foods, not drugsEven though many people take supplements because they want to improve their health, the FDA doesn’t regulate them as medications but instead as foods, under the Dietary Supplement Health and Education Act of 1994. “What happened in 1994 was that all of these products from vitamins, minerals, to botanical extracts became subcategories of food,” explains Cohen. “It also created a completely different structure in terms of advertising, like the ability to advertise products to say things like ‘This will boost your immune system’, as code for ‘This will prevent infection,’” he says. Manufacturers are not required to prove that their supplements are effective or safe before they market them. And supplements are not held to the same manufacturing standards as drugs, which can lead to adulterated or substandard products. “It’s basically very difficult, if not impossible, to separate poor-quality products from higher-quality ones in the market, at least at present,” says Cohen. Part of the problem is that the current system doesn’t do a good enough job of tracking when supplements cause harm, says Cohen. “I think we have to realize that for the public to have access to high-quality vitamins and minerals and botanicals, we’re going to need to reform the law,” he says. Cohen has previously suggested changes to the current regulations, including standardizing manufacturing processes, carefully vetting new ingredients, and creating higher standards for the claims manufacturers can make about their supplements. But for now, consumers can keep a few things in mind when deciding whether to take supplements. Navigating the supplement aisleWhen evaluating supplements, be wary of extravagant claims, as they’re unlikely to hold true. Also be aware that some supplements may contain a much higher dose in a single pill or serving than you need. “Sometimes these supplements are promoted at doses that are much higher than what you would get with diet,” says Guallar. In general, consult your doctor about any supplement use, as many supplements can interact with medications you’re taking. They may also not be safe to take while pregnant or breastfeeding, before a surgery, or during cancer treatment or other medical treatments. Consumers should also know how to spot poor-quality products. “My general advice to patients is to stick to supplements that list only one ingredient, and avoid a mixture of things, with the exception being multivitamins,” says Cohen. He cites certain certifications, such as USP or NSF International, as a sign of higher-quality products. Watch out for weight-loss supplements, muscle builders, and sexual enhancers, which previous investigations have found are sometimes adulterated with illegal or obscured ingredients, such as pharmaceutical drugs and synthetic chemicals. These types of supplements may be particularly susceptible to containing these undisclosed ingredients. Finally, consumers can look up information on specific vitamins, minerals, and botanicals on trustworthy websites, including those run by the Memorial Sloan-Kettering Cancer Center and the National Institutes of Health. The bottom line“We don’t eat a single nutrient; we eat a food,” says Zhang. “That’s why a lot of supplements don’t achieve the same effect as the natural nutrients coming from food sources,” she says. Zhang notes that the scientific evidence could always evolve as researchers continue to study nutritional supplements. But for now, there are more reliable ways to improve health. “Dietary supplement use shouldn’t be a substitute for a healthy diet and lifestyle,” says Zhang. “There’s no magic pill, unfortunately.” The lowdown on popular supplementsGenerally considered usefulFolic acid during pregnancy: Folic acid supplementation during pregnancy is well established to help prevent birth defects. “That’s considered a success story,” says Guallar. Fiber: Fiber supplements like psyllium may help reduce constipation, prevent heart disease, and lower cholesterol—though getting fiber from your diet also provides the vitamins and micronutrients found in whole foods. Melatonin: It may help with jet lag. However, the evidence that it helps with insomnia or sleep disorders is not particularly strong. Calcium and vitamin D after menopause: Postmenopausal women may benefit from taking calcium and vitamin D supplementation to prevent bone loss. A supplement mix for adults with age-related macular degeneration: A combination of zinc, vitamins C and E, copper, lutein, and zeaxanthin may help slow vision loss in people with this eye disease. Mixed or no evidence they helpMultivitamins: They’re extremely common—an estimated third of U.S. adults take them—yet there’s no clear evidence that they help reduce mortality or prevent major chronic diseases, such as cancer or heart disease, in healthy people. But experts say that multivitamins probably won’t hurt you, either. Echinacea: It may slightly reduce chances of catching a cold, but the evidence is weak, and there’s little proof that it helps treat colds or respiratory infections. Ginkgo biloba: Studies have found that this supplement does not seem to improve cognitive performance or prevent Alzheimer’s disease or dementia. Glucosamine and chondroitin: There’s mixed evidence they help ease symptoms of osteoarthritis. Vitamin D: Despite a lot of interest in its many potential health benefits, it’s still unclear if D supplements do much for healthy people. And in people who don’t have a deficiency, Zhang has found that very high doses of vitamin D may increase risk of all-cause and cancer mortality. Antioxidants: Comprising vitamins A, C, and E, as well as selenium, beta carotene, and folate, antioxidants have been touted as having numerous health benefits, but so far they have not lived up to the hype. They don’t appear to protect against heart disease, stroke, or cancer, and some may be harmful at high doses. Omega-3 fatty acids: Eating foods rich in omega-3 fatty acids, like fish, has been shown to protect against heart disease—but whether they offer the same protection when consumed in supplement form is still unclear. Some studies indicate that they may help protect against certain heart conditions, whereas others showed no benefit. from https://ift.tt/IWTbkS2 Check out https://takiaisfobia.blogspot.com/ A baby zebrafish is just half the size of a pea. A recent look inside its transparent brain, however, offers clues to the far bigger mystery of how we remember—and how we forget. In an experiment that yielded insights into memory and the brain, a team of researchers at the University of Southern California taught the tiny creature to associate a bright light with a flash of heat, a temperature change the fish responded to by trying to swim away. Using a custom-designed microscope, the team then captured images of the animals’ brains in the moments before and after they learned to associate the light and the heat. It’s the first known look at how a living vertebrate’s brain restructures itself as the animal forms a memory. [time-brightcove not-tgx=”true”] 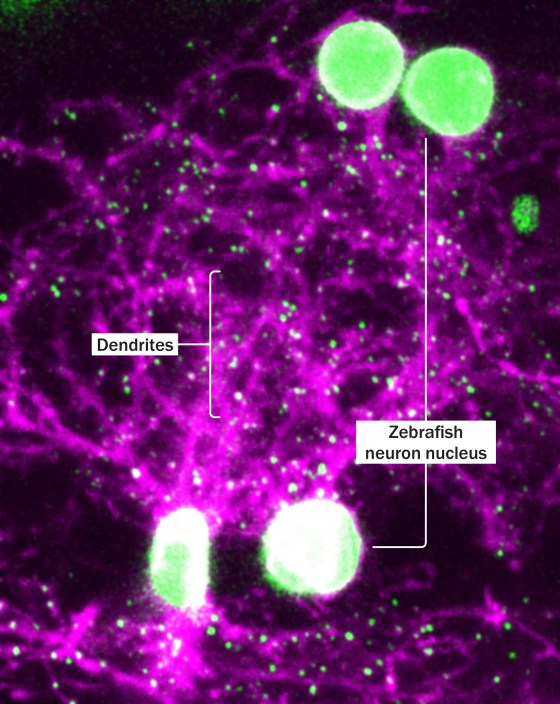
In the image published with the team’s research, the event looks like a dissipating firework. A frenetic spattering of bright yellow dots represents new connections created between brain cells at the moment the memory formed. But the image also shows a second, parallel force at work in the animal’s brain as those connections are made. An overlapping sprinkle of bright blue dots indicates synaptic connections that disappeared at the same time the new ones formed, as if the components of earlier zebrafish memories were making way for the new arrival. 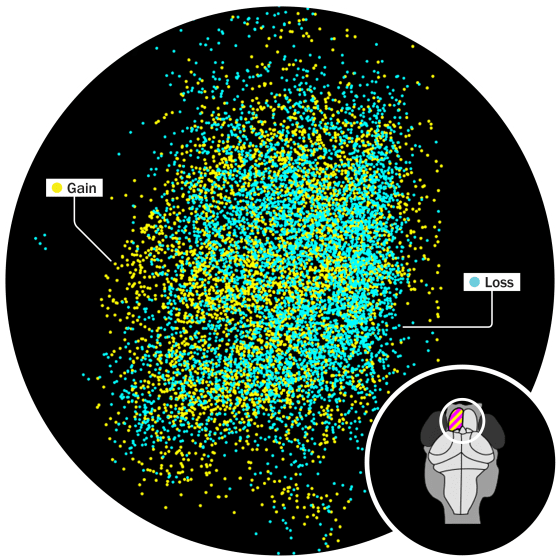
This glimpse into the mind of a zebrafish illuminates one of the most intriguing new fronts in science’s quest to understand the brain: the biology of forgetting. We often experience forgetting as a frustration—the misplaced wallet, the name just on the tip of your tongue. And until fairly recently, the widely held convention in neuroscience was that forgetting was merely a glitch in the memory system. The brain’s job was to gather and store information, and the inability to retain or retrieve those memories was a failure of some neurological or psychological mechanism. Over the past decade or so, however, science has determined that forgetting is not just the failure of memory but its own distinct force. “We were all taught forever, everyone, that forgetting is a passive breakdown of the memory mechanisms,” says Scott A. Small, a professor of neurology and psychiatry at Columbia University and author of the 2021 book Forgetting: The Benefits of Not Remembering. “The fundamental insight—the eureka, I think, of the new science of forgetting—is that our neurons are endowed with a completely separate set of mechanisms … that are dedicated to active forgetting.” The brain forms memory with the help of a complex tool kit of neurotransmitters, proteins, and carbohydrates, as well as other cells, Small writes; forgetting, too, has its own set of dedicated molecular tools working to clear away what’s no longer relevant. The mere existence of these neurobiological tools doesn’t prove that they’re useful; nature also gave us the appendix, and we’re still trying to figure out what the point of that one is. But a “constellation of findings” in recent years, Small says, indicates that culling the vast amount of information the brain collects and encodes is a necessary function of cognition—as essential for survival as the gathering of useful knowledge. And now that we know this culling function exists, some researchers are exploring the possibility that disruptions to forgetting could provide insights into complex psychological conditions like post-traumatic stress disorder. After all, forgetting, says Oliver Hardt, an assistant professor of psychology at McGill University, is “one of the most fundamental aspects of a memory system. Without forgetting, nothing would work.” The Nobel Prize–winning neuroscientist Eric Kandel, a professor of biochemistry and biophysics at Columbia University, established in the 1970s that changes in the chemical signals between neurons were the biological basis of all learning or memory making. When neighboring brain cells, or neurons, are excited at the same time, neurotransmitter chemicals fire across the microscopic gap between the ends of the neurons’ spindly dendrites. This change in the synapse—the connection point—between neurons is what makes a memory. For transient short-term memories, that change is fleeting. The more a memory is revisited and repeated, however, the stronger and more enduring that change becomes. That’s true of all animals capable of learning, Kandel found, from humans to the humble zebrafish. (“Practice makes perfect,” Kandel said in his Nobel lecture, “even in snails.”) If all animal brains are capable of forming new synaptic connections, it stands to reason that they’re also equipped to pare those connections away. That picture of the zebrafish brain illustrates the simultaneous creation of new synaptic connections between some neurons, and receding connections between others. Read more: How Social Media Is Hurting Your Memory From an evolutionary perspective, the purpose of memory “is not to allow us to sit back and say, ‘Oh, do you remember that time?’” says Sheena Josselyn, a senior scientist at the Hospital for Sick Children, and a professor of psychology and physiology at the University of Toronto. “It really is to help us make decisions.” Without forgetting, the evolutionary benefits of a strong memory would become redundant, says Hardt. In the course of a single day, the brain registers hundreds of thousands of bits of information, some of it relevant and much of it utterly inconsequential: the way your socks felt when you pulled them onto your feet, the shirt color of a stranger standing before you in the grocery-store line. “You would have an endless amount of useless stuff accumulating there constantly,” Hardt says. “And each time you want to think about something”—something key to your survival, such as the location of food or the signs of an approaching predator—“all these memories would pop up that are completely meaningless and that make it hard for you to actually do the job of predicting what is next.” Hardt is among the many scientists who suspect that this culling of nonessential memory is one of the key purposes of sleep. A good night’s sleep quite literally produces a clearer mind. Josselyn and her spouse Paul Frankland run the Josselyn Frankland Neurobiology Lab at Toronto’s Hospital for Sick Children. Frankland’s research at the hospital has focused on the kind of forgetting that takes place in the hippocampus when new learning takes place—the corresponding gain and loss of neuronal connections that the zebrafish brain showed. Frankland’s breakthrough in forgetting came while he was studying neurogenesis, or the formation of new brain cells, in mice. A graduate student noticed that the more quickly new neurons formed in the animal’s hippocampus, the less likely the animal was to recall some older memories. Mice with more brain cells learned new mazes faster, but they were also more likely to forget the layouts of previous mazes they had mastered before their brain growth. Frankland has theorized that’s why it’s so difficult for people to remember events from early infancy, a time of exponential neural development. In this model, forgetting in the hippocampus isn’t a zero-sum, one-for-one replacement of knowledge, so much as an ongoing reconfiguring of memory so that more recent (and likely, more useful) information is available more readily. “The world changes,” Frankland says, “and so the more recent things are more relevant to remember to predict the future than the more distant things.” Just as the brain’s cells and circuits distinguish between long- and short-term memory, there also appears to be a distinction between memories that have decayed beyond the possibility of retrieval and what researchers call “transient” forgetting—the temporary (if deeply irritating) inability to recall a piece of learned information. Read more: Why People With Anxiety May Have Better Memories Studies in fruit flies, most notably in the Scripps Research Institute lab of neuroscience professor Ronald L. Davis, have identified dopamine as a key factor in the animals’ ability to learn and forget. Last year, the lab found a dopamine-releasing circuit in the flies’ brains linked to transient forgetting. Flies that had been taught to associate a particular odor with a shock to their feet seemed to forget what they’d learned when distracted by stimuli like blue light or a puff of air. This temporary loss of memory was accompanied by the release of dopamine from a particular set of cells onto the cells thought to hold memory. If fruit flies have a mechanism that temporarily suppresses some memories, it stands to reason humans do too. “Forgetting may be the basal state of the brain. We are inundated with so much information on a daily basis that the brain fights back and says, ‘I can’t handle this. I need to forget as much of the unimportant information as possible,’” Davis says. “The brain is designed to slowly erase information that’s coming in on a daily basis unless consolidation says, OK, this memory is important. And so it overrides the forgetting mechanism.” As the neuroscience of forgetting emerges, some researchers are questioning whether the mechanisms that regulate forgetting might also hold valuable clues to other mysteries of cognitive and behavioral health. In his book, Small points to a few key areas in which the neuroscience of forgetting might point the way to other breakthroughs. One area of interest is autism. In one 2016 study, when a protein associated with forgetting was inhibited in fruit flies, those that had been modified to contain genes linked to autism demonstrated “behavioral inflexibility,” or difficulty adopting new patterns of behavior. The aversion to excess stimuli that some people with autism spectrum disorder show, Small says, could be the result of a brain unable to let go of unessential inputs. Post-traumatic stress disorder, likewise, could be the result of an injury to the forgetting function. One theory is that PTSD develops as a result of an overgrowth of synaptic connections in the amygdala, the part of the brain that acquires and stores fear memories, after intense or repeated exposure to a frightening stimulus. Early studies show that drugs that accelerate the loss of fear memories--most notably, MDMA—could be effective in treating the symptoms of people with PTSD. The memory loss associated with Alzheimer’s disease and other forms of dementia ranges far beyond the kind of routine forgetting that takes place in a healthy brain. Yet understanding the minute physical processes behind the undoing of memory could help researchers understand more about this most painful symptom of the disease, and maybe even find ways to slow or stop it. “Perhaps we need to understand the forgetting process, how that works, why it is there, in order to find a better way to address it if it goes out of control,” Hardt says. Several researchers interviewed for this piece referenced the Jorge Luis Borges short story “Funes the Memorious” to illustrate forgetting’s role in how we navigate the world. An injury sustained in a riding accident leaves the title character with a chronic inability to forget anything at all. Funes learns multiple languages with ease and can cite millennial–long strings of historical facts—the kinds of things we think we’d do with infinite capacity for recall. But he’s miserable. Funes can’t let go of anything. He looks at a landscape and registers every leaf on the vines, every hair in a pony’s mane. He’s swamped by minute changes of age and expression each time he looks at another person’s face. Memories don’t comfort him; they only overwhelm. “My memory, sir, is like a garbage heap,” Funes tells the narrator. Forgetting serves us well. It tunes out useless information so we can focus on the relevant. Without it, neither anger at a slight nor the pain of grief would fade; feelings of love and attraction would not either, making it impossible to move on from relationships. Memories build us, and forgetting chisels away the excess, shaping the way we see ourselves and our world. from https://ift.tt/f6IOu1k Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
