|
Before the pandemic, about 1,000 new patients came to Boston’s Dana-Farber Cancer Institute for treatment consultations each week. When COVID-19 hit Massachusetts this spring, the number of new consultations fell by half and the hospital moved as many appointments as possible online. Now, with daily case counts relatively low in the area, the hospital is back to scheduling about 800 consultations per week, using a mixture of telemedicine and in-person appointments, says associate chief medical officer Dr. Andrew Wagner—but that still means about 200 cancer patients per week are not getting the treatment consultations they would in more normal times. Continued travel restrictions and fear of infection likely play a part, but many would-be patients aren’t setting up appointments because they don’t know they need to. The number of cancer screenings happening nationwide plummeted this spring when lockdowns went into effect, meaning many of the people who would be seeking care from Wagner and his colleagues don’t yet know they have cancer at all. “Five months in, with the procedures and equipment we have put in place to ensure the safety of our patients and our staff, the potential health impact from [canceling cancer screenings] is a bigger concern than the pandemic,” Wagner says. When COVID-19 hit the U.S. this spring, hospitals in many areas canceled elective surgeries to redirect resources and personnel to treating coronavirus patients, and people were encouraged to use telemedicine or delay non-urgent medical appointments. While doing so was necessary to try to stop the spread of the virus, it led to unintended consequences. About 40% of Americans recently said they were unable to get some kind of care due to the pandemic, and studies show emergency room visits plunged nationwide. For cancer patients, the unintended consequences start with those who don’t even know they have the disease yet. Studies suggest the pandemic led to a roughly 80% drop in routine screening appointments that could catch new cancers in March and April. Rates recovered somewhat in the late spring, but one paper still estimated approximately 60% fewer breast, colon and cervical cancer exams from mid-March to mid-June compared with years prior. That translates to hundreds of thousands of missed exams nationally—and, among those who do have undetected cancer or precursors to it, the loss of potential early diagnoses and interventions. Part of the problem, Wagner says, is that the vast majority of cancer screenings can’t happen virtually. Most screenings require an in-person procedure like a colonoscopy (for colon cancer), mammogram (for breast cancer) or a pap smear (for cervical cancer). Some clinics can test for colon cancer with a stool sample patients send in from home, and dermatologists may be able to look at an unusual mole remotely—but that’s about where the list ends. Even remote tests for colorectal cancer aren’t used as often as they could be, says Dr. Rachel Issaka, a gastroenterologist and clinical researcher at the Fred Hutchinson Cancer Research Center in Seattle. “In this era of social distancing, this really is an opportunity for us to start to use these tests to a greater extent,” Issaka says. “This time is requiring us to be a little bit more creative.” The stakes are high. Fewer screenings translated to fewer cancer diagnoses during the pandemic, data show. According to one estimate, the number of weekly diagnoses for breast, colorectal, lung, pancreatic, gastric and esophageal cancers dropped by about half during the pandemic. The U.S. Preventive Services Task Force sets specific recommendations for who needs which screening tests, and how often. Most cancers are slow-growing enough that missing those intervals by a few months won’t make a huge difference, says Dr. David Cohn, chief medical officer at the Ohio State University Comprehensive Cancer Center. “But the biggest fear is that a couple months turns into a couple years,” he says. If a cancer goes undetected for years, the patient’s prognosis could be grim, he says. Patients who had been diagnosed prior to the pandemic have experienced disruptions, as well. The U.S. Centers for Disease Control and Prevention never recommended that people with a cancer diagnosis delay their care, but cancer patients and their doctors have had the difficult task of weighing the risk of COVID-19 against the urgency of cancer treatment. As TIME reported last month, some patients have deferred chemotherapies and radiation treatments that need to be administered at medical facilities under professional supervision. In one April survey of breast cancer patients, 44% reported treatment delays during the pandemic—a number that was relatively steady regardless of the stage of cancer. The highest rate of delays concerned routine follow-ups and breast reconstruction surgery. But about a third of respondents reported delays in cancer therapies that take place in a medical facility, including radiation, infusion therapies and surgical tumor removal. It’s too soon to say what the fallout from all the delays in screenings, diagnoses and treatments will be. Dr. Ned Sharpless, who leads the National Cancer Institute, which is part of the U.S. National Institutes of Health, estimated that pandemic-related delays in screenings and cancer care will over the next decade result in about 10,000 excess deaths (on top of the 1 million typically expected deaths) from breast and colorectal cancer alone. The analysis of these two cancers, which account for about a sixth of all cancer deaths, is based on a conservative model that assumes pandemic-related delays last only six months. “Even a small dropoff has a very substantial impact on population health,” Cohn says. We won’t see these deaths show up in the data for a few years, since many cancers progress in severity over a relatively long period of time. Most hospitals and doctors’ offices are again encouraging patients to come in for routine care. Many have implemented safety protocols (like limitations on visitors, getting rid of waiting rooms and mandatory COVID-19 testing for certain patients and staff) that make it safe for most patients to come in for screening tests, Cohn says. And there is at least one way telemedicine can help cancer care, Cohn says. Patients who are nervous, or who have unique risk factors, can talk through the risks and benefits of making an appointment with their doctor first, from home. from https://ift.tt/3b6Hu3d Check out https://takiaisfobia.blogspot.com/
0 Comments
There are no easy answers to the questions about bringing kids back into classrooms this fall. Parents, school administrators and educators must instead weigh two bad options: isolate children at home or risk them getting and spreading COVID-19 through in-person contact. That decision is daunting even for infectious disease experts and epidemiologists. Over the last few months, they have been forced to think about the pandemic not only as scientists and scholars, but as parents, and despite their wealth of knowledge, like any parents, these experts are grappling with uncertainty. There are ways to limit the spread of the COVID-19, including masks and ventilation, but there is no way to guarantee zero risk of disease transmission in schools. At the same time, remote learning can exact its own toll, setting back children’s mental health, academic achievement, and social development, and leaving their parents exhausted and demoralized. In interviews with TIME, 10 experts explained how they’re trying to strike a delicate balance: between their children’s academic and emotional needs; the risk to their communities; keeping their children and their families safe from the virus; and trying to preserve their own sanity and careers. Dr. Joshua Barocas—infectious disease physician and assistant professor of medicine at Boston University School of Medicine at Boston Medical CenterBarocas’s 7-year-old son and 3-and-a-half-year-old daughter are enrolled in second grade and preschool, respectively, at Boston public schools. The school year at Boston public schools has been delayed until Sept. 21, and, initially, all learning will be remote; the school district will then phase in a hybrid model combining in-person and remote classes starting in October. Barocas plans to start sending his children to school in-person as soon as it’s available—so long as the positivity rate in their neighborhood does not start to rise. “We can only control what we can control. I don’t have some magic wand that can make the school district do everything that I want them to do. So can my kids protect themselves? As an infectious disease physician who’s been dealing with COVID since the very beginning, my kids have learned how to wear a mask properly and even though it’s uncomfortable, they do it. And it was something they have made a habit of. They’ve also been doing a lot of hand-washing, and they have been sort of taught and reinforced that at this point, we need to give people space … In all of those discussions, we made it clear that this was not just to protect themselves, but to protect other people as well.” Tara Smith—professor of epidemiology at Kent State University College of Public HealthWhile her local school district was offering a hybrid option, Smith decided that her 6-year-old son, a first grader in Kent, Ohio’s school district, will attend all-remote classes. Meanwhile, her 18-year-old son was slated to attend Kent State this fall, which is offering mainly remote courses, but has decided to delay starting college because he found it difficult to learn remotely. “I feel that transmission is too high here. We don’t have it under control. We still don’t have enough testing, and I just did not feel comfortable sending [my younger son] back to school in person … I thought since we had the ability to school him [at home], that for other parents that don’t have that option, this would be one less child that was in the classroom, and give them a little bit more space.” Kimberly Powers—associate professor of epidemiology at University of North Carolina Gillings School of Global Public HealthPowers’ three children ages 11, 9, and 5, will be remotely attending sixth grade, fourth grade and kindergarten, respectively, at a charter school in Hillsborough, N.C., which has gone all remote at least through mid-October. She had been involved with the school’s planning for the fall, and had initially advocated for the school to have in-person classes for students in kindergarten through fourth grade, but ended up agreeing with the school’s decision due to the increased level of community spread in North Carolina in recent months. “I do think ultimately the decision to hold off on reopening was a prudent one, at least from a transmission-prevention standpoint. But obviously, there are so many negative repercussions outside of just the coronavirus to consider when choosing what to do. It’s hard to feel great about any option they could have selected.” Dr. Alison Rustagi—resident physician at the University of California, San Francisco Medical Center who has a Ph.D. in epidemiologyFor the coming school year, the San Francisco Unified School District plans to employ only distance learning, so Rustagi’s 7-year-old daughter, a second grader, will be learning from home; the family plans to hire a nanny to help out. Rustagi originally planned to send her other daughter, a 2-year-old, to a private preschool, but ultimately decided that the risk and financial expense was too great. “In a community in which there’s ongoing, widespread, sustained community transmission, I think that the burden generally has to be on proving that it is safe to return to school, rather than proving it’s unsafe to resume school.” Dr. Sarah Doernberg—associate professor in the Division of Infectious Diseases at the University of California, San Francisco Medical CenterDoernberg’s 6-year-old and 8-year-old, like Rustagi’s children, are in the San Francisco Unified School District, which has gone all-remote. But in their case, both will attend an “on-site learning camp” with counselors provided by UCSF, where they will gather with small groups of other children in-person; these small groups, in turn, will connect remotely with others in their grade level for online learning. “To be honest, I would have felt comfortable sending my kids back now with having kids spaced apart, enforcing mask wearing, and if they could educate—as much as possible—outdoors … I think there’s risk in everything we do in life, and there’s some risk to sending them to school during the pandemic, but I think the potential benefits for getting kids back to school are really great.” Lisa Bodnar—professor of epidemiology at the University of PittsburghBodnar’s three children attend fourth, seventh and 10th grade in the Mount Lebanon School District near Pittsburgh, which will begin the school year all-remote. She says distance learning this past spring “was not a good learning experience” for her children, but feels encouraged by the schools’ efforts to add more structure to the digital school day this fall. “I’m much more hopeful that the kids will have a better experience learning, that it will be closer to what it could be in school. I know that they will be safer. I am not fully convinced that all of their needs will be met.” Jamie Lloyd-Smith—professor of ecology and evolutionary biology at the University of California, Los Angeles professorLloyd-Smith’s son, 4, and daughter, 6, both go to a school in Santa Monica that has gone all remote. His son would normally be in preschool; instead, he will be in a “pod” with two other children, led by an assistant teacher. The pod will meet outdoors (with masks on) for three hours every morning. His daughter will be doing some play and some academic work with three other children and a teacher several afternoons a week in-person in the families’ backyards, in addition to remote learning. “As a parent, even though I understand that the risk to younger children from COVID is quite low, there are exceptions to that. And so as a parent, of course, that’s always on your mind. You don’t want to put your child at risk, even if it’s a low risk.” Sandra Albrecht—assistant professor of epidemiology at Columbia University Mailman School of Public HealthAlbrecht’s 5-year-old daughter will be attending kindergarten in Queens; her school is using a hybrid model, in which the class is split into two groups, and each goes into the classroom two or three days each week on an alternating basis. She says that with the low rate of community transmission in New York City, combined with her daughter’s needs and the precautions at her school—including masking for everyone—she feels “quite comfortable” sending her to school. “For my daughter, it was hands down. It wasn’t even a debate, actually. We selected the hybrid model, and to be honest, if the five day in-person model was available, we would have selected that … A lot of the learning happens in terms of interaction. There’s a lot of socio, emotional type of learning that happens at that age. And it’s just very difficult to deliver that kind of education through remote outlets.” Whitney Robinson—associate professor of epidemiology at University of North Carolina Gillings School of Global Public HealthRobinson has kept her sons, 18 months and 5 years old, in daycare through most of the COVID-19 outbreak. Her older son is attending kindergarten in the Chapel Hill-Carrboro City school district, which has gone all-remote through January; during that time frame, he’ll still be attending in-person daycare, while also taking remote classes provided by the public-school kindergarten. “I was more concerned about … posing a danger to these teachers versus a danger to my children. I decided that given the restrictions they’ve put in [at his school], they’re following all the state mandates and being pretty careful, I felt comfortable with it. But I’ve also made decisions that we’re not seeing other family members, that we ourselves are not socializing with other people outside the school unless it’s masked or outside, distanced. Because we want to make sure we don’t become a vector of transmission for people in the school.” Eyal Oren—associate professor of infectious disease and social epidemiology at the San Diego State University School of Public HealthOren’s sons, ages 12 and 9, are entering sixth and fourth grade, respectively, in the San Diego Unified School District, which plans to be all-remote initially, but is discussing shifting to a hybrid model later on. He says that he would consider sending his children to in-person classes, but will weigh in many different factors—including his sons’ differing personalities and whether there will be distance between children, and if they will spend substantial time outside. Parents must “look out for their own family” and make their own decisions given all the uncertainty, says Oren. “I need to be convinced by my very particular school and teacher and so on that they know what they’re doing. That for me is important. Not just the broader district saying, ‘here’s what we’re doing.’” from https://ift.tt/2EE5dLY Check out https://takiaisfobia.blogspot.com/ An Aug. 26, the U.S. Food and Drug Administration (FDA) gave an emergency use authorization (EUA) for a rapid COVID-19 test that can produce results in just 15 minutes, which could not only increase the number of people tested in the U.S., but also identify those who are positive sooner, so they can self-isolate and limit spread of the disease. The testing device, made by Abbott Laboratories and called BinaxNOW Ag Card, is about the size of a credit card and can be easily used anywhere people need to be tested. It analyzes samples from a nasal swab and comes with an app that people can download to receive their results—which could serve as verification that someone is free of infection for schools, employers and other venues where a larger number of people might gather. Any doctor who suspects a patient may have COVID-19, based on their exposure history or symptoms, can write a prescription for the test. The test, which needs to be performed by a doctor, nurse, school nurse or occupational health professional, picks up specific proteins made by SARS-CoV-2, the virus behind COVID-19. Using a quickly generated readout similar to that in pregnancy tests, the self-contained test opens up like a billfold for the health care provider to insert the nasal swab containing the sample. When closed, the built-in chemical reagents scan the sample for the viral proteins and produces a single band if the test is negative and double bands if positive. Because it focuses on these proteins, the test is most effective when used on people within days of infection, when the virus is actively infecting cells and churning out viral proteins. Abbott conducted trials of the test at seven sites in the U.S. on people suspected of having COVID-19, all tested within seven days of their first symptoms. In those studies, the sensitivity of the test was 97.1%, meaning it can pick up positive cases 97.1% of the time with few false negatives, and its specificity was 98.5%, meaning it correctly identifies people without infection as negative 98.5% of the time, with very low false positives. The gold standard for COVID-19 tests, known as the PCR test, amplifies genetic signatures of the virus itself, so it can read positive during and even well after infection, if there are any traces of dead, inactive virus remaining. The latest data also suggest that the PCR test can produce false negatives, since the threshold for picking up these genetic signatures is sometimes not sensitive enough if levels of the virus are too low. While the sensitivity of the Abbott test is slightly below that of the PCR test, “any drop in sensitivity compared to the PCR test is more than made up for with the fact that the [Abbott] test is repeatable,” says Joseph Petrosino, professor and chair of the department of molecular virology and microbiology at Baylor College of Medicine who was not involved in the development or testing of the BinaxNOW. “If you are taking this test every other day, or twice a week, then you can be pretty confident that something that went wrong one day wouldn’t go wrong the second day.” Testing the same group of people—like all the students at a given school, or residents of a specific nursing home—multiple times in quick succession is currently a luxury in the U.S. At the moment, it can take several days or even weeks for results from PCR tests, and those delays are contributing to problems in containing infections. Testing people regularly could be useful in identifying and isolating those who are positive sooner, reducing their chance of spreading COVID-19. That could be critical to containing outbreaks as schools reopen and people return to work. Admiral Brett Giroir, the U.S. assistant secretary for health who is overseeing the country’s testing efforts, tweeted that the quicker turnaround for results from the test would be a “game changer.” The cost of the Abbott test is also a plus; at $5, it could be more accessible to more people, although many insurers currently cover the cost of COVID-19 testing. Since April, Abbott has built two new facilities to manufacture BinaxNOW and plans to ship tens of millions of test in September, and scale up to producing 50 million tests each month by the beginning of October. from https://ift.tt/3jiMPHw Check out https://takiaisfobia.blogspot.com/ Mental health flows from the ceramic jug psychotherapist Lori Gottlieb keeps on her desk. There’s nothing special about the jug—a minor accessory in an office designed with the sort of tidy impersonality common to her field. And there’s no special elixir in it—just water. But all the same, the jug provides a certain kind of healing. When patients are struggling, crying, overcome in some way, Gottlieb, a Los Angeles based practitioner and author of the book Maybe You Should Talk to someone, will offer up a cup of water, pour it for them and hand it across. In that small gesture is a whole constellation of meaning: concern, care, protectiveness, generosity. It’s a little grace note that’s possible only in person—only when two people are in the same room, sharing the same space, face to face across just a small physical gap. Ever since March, however, when much of the U.S. went into lockdown as a result of the COVID-19 pandemic, such in-office intimacy became impossible across nearly all professional disciplines. Psychotherapy sessions—like so very much else—have become virtual, conducted on-screen, at a remove, riding the electrons of Zoom or Skype or Google Meet. And that comes at a price. “There’s the ritual of coming in every week, sitting in that room on the same spot on the same couch in the same office,” says Gottlieb. “It feels incredibly comforting and safe. I think the environment part of it is very important for people.” That’s not true just of mental health, of course. Most of us aren’t getting a fraction of the person-to-person interaction we’re accustomed to, and most of us are pretty well fed up with it. Virtual birthday parties are no party at all. Virtual happy hours have everything but the happy. Call it Zoom fatigue, cabin fever, flat-out loneliness—many today are suffering from isolation to one degree or another and long for the moment that the virtual lives we’ve been forced to live can be tossed aside. But telepsychology (or telepsychiatry or tele-mental-health, as it’s been variously called) may have a stickiness to it that other aspects of virtual living lack. In recent years there’s been more and more talk in the health care professions about the potential for telemedicine. For some kinds of care, it’s easy to see how routine “office visits” that allow doctors and patients to meet without the need for an actual office could work: the orthopedic surgeon checking a patient’s range of motion and inquiring about pain after knee replacement surgery, say. But too many other visits require hands-on contact—palpating, blood draws, suturing—to make telehealth a universal practice. Tele-psych, though—with its talk-and-listen simplicity—is a different matter. If ever there was a caring discipline that was poised to jump aboard the telemedicine train, it’s mental health. “In February of 2020, before COVID-19 really hit our country, telepsychiatry was beginning to be widely available but only sporadically adopted,” says Dr. Jay Shore, a professor at the University of Colorado Anschutz Medical Campus and the chair of the American Psychiatric Association’s Telepsychiatry Committee. “Now it’s been a tsunami. At the University of Colorado maybe 10% to 20% of [mental health] visits were over video before. Now, outside of inpatient stuff, we’re at like 100%.” That has been true pretty much everywhere else in the country, where therapy sessions have been happening either online or not at all. In mid-May, the American Psychiatric Association surveyed its members on how frequently they held tele-psych sessions both before and after the onset of the pandemic. The results were striking: Prior to COVID-19, 63.6% of respondents did not use virtual sessions at all. After the onset of the pandemic that figure plunged to just 1.9%. Conversely, before COVID-19 hit, only 2.1% reported using tele-psych 76-100% of the time. During the pandemic that figure has soared to 84.7%. It was a change made by necessity, not by choice, but there are plenty of people who like what they’re experiencing. There’s convenience for one thing: a 50-minute session is a 50-minute session, not two or three times that as the patient wastes part of the day just getting to and from the appointment. That’s especially important in rural communities that might have been mental health deserts before—with the nearest caregivers requiring a long drive to the closest big city. Patients are able to have their appointments pretty much anywhere. “If you were going to go drop your kids off at soccer practice, you could sit in the car and have a relatively private session with your therapist while you’re waiting for the soccer match to be over,” says psychologist Jared Skillings, chief of professional practice for the American Psychological Association. “This provides a significant increase in access and quality of life.” Tele-psych also allows for more enduring doctor-patient relationships. If your job transfers you to another city, you can always find another doctor to tend to your physical ills, but you didn’t spend years confiding your most intimate secrets to your cardiologist or ophthalmologist and now have to start over with an entirely different person. Your psychologist is another matter entirely. “The advantage is clearly that you get to have continuity of care,” says Gottlieb. All of those plusses have some in the community convinced that not only are tele-sessions the future of mental health, but that that future is now. “I think that anyone who tries to prognosticate comes across as a fool,” says Shore. “But what I can say is that we will never be the same, we won’t go back to where we were.” And yet, what about that water jug? What about the sense that a therapist’s office is a third place, a safe space, neither work nor home but a place that, for those 50 minutes at least, feels like the patient’s own? Not every patient is the same and for many there is a comforting ritual in the opening of the doctor’s door and the gathering in that follows. Shore may indeed be right that the forced experiment with tele-psych that the quarantine months have necessitated has dramatically changed the game. Just how much and how enduringly it’s been changed is the real question. Teletherapy may seem very much of the moment, but it’s not a new idea. As long ago as 1959, the University of Nebraska began a pilot project using mid-century video technology to allow patients and doctors to meet remotely. But the system was expensive and impractical and it lent itself poorly to the Freudian era of lying on couches and free-associating to a silent therapist whose face you didn’t even see. It wasn’t until the late 1990s, with the Internet fully entrenched and two-way video platforms coming online that the telehealth gained any traction. Even then though, it was used in a limited way. “We started to see big systems like the Department of Defense and the Veteran’s Administration and jails develop sustainable larger scale telepsychology services to serve their populations,” Shore says. Still, that was enough to prove the technology’s potential—if not its immediate appeal—and practitioners adopted it unevenly. While Shore reports that well before the pandemic he already had patients he’d worked with for 12 to 15 years and had never met in person, Gottlieb wanted no part—or at least very little part—of telehealth. “I didn’t do telehealth at all unless there was a circumstance like I already had an established patient and that person was going to be on a work assignment for a few months,” she says. “But I would never meet somebody doing telehealth.” Then the pandemic forced the profession’s hand and even doubters like Gottlieb have seen some of its advantages. She concedes that she likes the leveling effect of both patient and doctor getting background glimpses into each other’s homes—a sort of intimate equality of behind-the-scenes access. She likes the insight she gets when a patient Zooms from a bedroom and she catches sight of what’s on the nightstand. “Usually what people keep on their nightstand tends to be the most personal of things, what means the most to them,” she says. And she likes, too, the spontaneity and humor that a tele-session can provide. A surprising number of people, Gottlieb says, will have a session in the bathroom, sitting on a closed toilet—looking for a private spot in their homes. During one session, a patient was crying because her mother was in a nursing home where COVID-19 had been detected, and she was worried. She sat back and accidentally hit the handle of the toilet causing it to flush loudly. “She was embarrassed and said, ‘Am I the only person who does therapy from the toilet?’ And I said, ‘No, actually the toilet has become the new couch.’” They both laughed—which the patient later said was the best and most helpful moment in the session. Whether all sessions will be so effective depends at least in part on the kinds of issues the patient is struggling with. Obsessive-compulsive disorder, for example, lends itself comparatively well to tele-psych sessions because the standard of care for it is what’s known as skill-based therapy—learning behavioral tools that help break the OCD cycle—which may require less intimacy than other kinds of therapy, and instead calls for rigorous practice and discipline. Post-traumatic stress disorder patients may similarly benefit from online therapy, at least at first, since the home might feel like a safer space than a doctor’s office. But there are downsides in treating these and other disorders online—in the form of cues missed due to the limited frame of a computer screen. The jiggling foot, the knotted hands, the subtle shifting in the chair that telegraphs unease with a topic of conversation are all lost to the doctor in tele-sessions. For patients battling substance abuse it’s hard to get away with the telltale gait of intoxication or the smell of alcohol on the breath in an in-person session. Not so hard on Zoom. Group therapy can present its own challenges. A key part of the dynamic of the group involves eye contact—who’s listening, who’s not, who’s offering an affirming nod or shifting uncomfortably at someone else’s story that may hit a raw nerve in the listener. On a Zoom screen with a dozen faces arranged in Brady Bunch tiles, all of that is missing. Even when the group is just two people, things get lost. Gottlieb recalls counseling a couple in a telehealth session and suddenly noticing their mood going from comparatively detached to warm and compassionate. “I was trying to figure out what had shifted there and then one of them said they were holding hands,” she says. “But I didn’t see it. They were holding hands under where I could see.” If tele-psych is going to have a wide, post-pandemic future, it depends on more than just the acceptance of patients and providers. As with so much else in the U.S. health-care system, things come down to who will pay. During the pandemic, Medicare, many state Medicaid programs and commercial insurers have loosened rules or allowed waivers to cover telehealth sessions. When the pandemic ends, however, so could the payments. Those in the field want to stop that from happening, making sure we don’t lose the lessons we’ve learned from the experience. “We are advocating for Medicaid, Medicare, and private payers to keep telehealth turned on at least for 12 more months after the coronavirus pandemic is officially declared to be over so that we can better evaluate the impact that has had on patients,” says Skillings. In a live June 9 event with STAT News, Seema Verma, the Administrator for the Centers for Medicare and Medicaid Services (CMS), offered support for that kind of sentiment, arguing that coverage for most forms of telemedicine, including tele-psych, should indeed continue after the pandemic ends. The dramatic increase in overall access to care—with telemedicine visits increasing 40-fold in some parts of the country during the pandemic—is, all by itself, an argument for maintaining the system, she said. In August, the CMS issued new guidelines that provide physicians nine new billing codes to cover telemedicine going forward. The portability issue is another unsettled question that will endure beyond the pandemic. It’s true that one of the advantages of tele-psych is that patients who move from state to state can continue to work with their original doctor—but that’s only if each state’s licensing rules permit that kind of cross-border practice, and so far most don’t. In 2011, the Association of State and Provincial Psychology Boards—one of the profession’s governing bodies—created a task force to promulgate tele-psych guidelines for practitioners. From that came a proposal for what became known as PSYPACT, a national reciprocity system under which states would accord tele-psych privileges to practitioners living in other states. Joining the group requires action by state legislatures, and currently 15 have passed the necessary laws, with approval pending in 12 more states and the District of Columbia. “At the end of the day,” says Skillings, a vocal PSYPACT advocate, “this is actually about providing care to our community, to improve their health.” Improving community health is, of course, what all medicine, virtual or otherwise, is about. Mental health, which lacks the clarity of other medical disciplines—the blood tests and CT scans and MRIs that can make diagnosing illnesses and prescribing treatments so straightforward—has always needed more options in its therapeutic toolkit. Tele-psych, even with its doubters and its drawbacks, is easily one of the newest. In time, it may also prove to be one of the best. from https://ift.tt/3aZCSMh Check out https://takiaisfobia.blogspot.com/ Gardening has blossomed during the COVID-19 pandemic. Just as Americans planted “victory” gardens during wars and depressions before, now many are planting seeds to grow their own food. Doing so comes with real benefits, like stress relief, exercise and risk reductions for many diseases as a result of eating more vegetables. In a recent episode of TIME for Health Talks, Ron Finley, a Los Angeles–based urban gardener known as the “Gangsta Gardener,” and Questlove, a musician and food entrepreneur, talked about how gardening and the healthy foods it yields can also build community. A decade ago, Finley transformed the unused city-owned strip of land in front of his South Central, Los Angeles house into an edible garden for his community. Now, it’s such a popular spot that people swing by to help him plant, and others eat his juicy figs right from the tree. The point is to bring people together and give everyone access to fresh, organic food. “If you grow together, you grow together,” he says. “That’s what communities do.” Too many neighborhoods in the U.S. don’t have grocery stores or restaurants—let alone community gardens—that offer fresh, healthy and affordable food. “Where I grew up, there was no type of health options whatsoever,” says Questlove, who is from West Philadelphia. “I see this as a state of emergency. I almost feel like it’s invisible warfare on a community that doesn’t even know.” Finley now teaches people all around the world—Questlove is among his pupils—to garden through his popular MasterClass and through the Ron Finley Project. “Soil is my protest to all of these injustices that we’re dealing with, have been dealing with since the inception of this country,” Finley says. Here’s what Finley wants you to know if you’re new to gardening: Fear not.Newbies are not alone. “There are people…that have never touched soil in their life because it hasn’t been in their proximity,” Finley says. If kids can do it in kindergarten classrooms, so can you. “It’s soil, it’s water and it’s a seed and some air,” Finley says. “How difficult could it possibly be?” You don’t need acres of land to start.Lettuce, leafy greens and collard greens are all easy to grow without a lot of space, Finley says. You don’t even need a plot. “If it can hold some soil—if it’s a wooden crate, if it’s a shoebox—put some soil in it, put a seed in it, and start your garden.” It matters.“Knowing how to grow food is a life skill,” Finley says. “It’s in our DNA and we should nurture that DNA. That’s something that nobody ever can take from you.” Far from a frivolous hobby, growing your own food can change your life—and the lives of those around you. “What I’m finding out now is it’s bringing back the humanity in people.” from https://ift.tt/2ECY5Q5 Check out https://takiaisfobia.blogspot.com/ When publicized far and wide enough, infographics, some experts argue, can save lives. The communicative value in visualizing data towards improving public health outcomes is long-established, going back over two centuries. And while the earliest examples were intended to inform discussion and debate among an elite social sphere, they also sought to address real-world problems. From 1820 to 1830, an enthusiasm for statistics began to emerge across the western world, leading to an era of statistics concerned with reform. It was led by individuals who sought to disrupt what they saw as the chaos of politics and replace it with a new apolitical regime of empirical, observed fact. This new approach would come to be seen as a field of action, as an applied science, providing empirical weight to the new, intellectually dominant spirit of political economy. Following the creation of the General Register Office (GRO) in 1837, the first wave of statistical enthusiasm was applied to poverty and to the lived environment of the poor; the progressives who undertook these surveys did so in the legal context of the reforming acts of the early 1830s. Separate from (but at the same time, often socially or professionally connected to) the governments of this era, a network of liberal-minded, reforming individuals hailing from business and professional classes busied themselves in statistical pursuits. Within a few years, in the capital and in the major cities of the industrial north, a series of societies was founded, each bearing the imprint of their own members’ interests and concerns. Health matters tended to dominate the concerns of the societies in part because health represented “a fundamental component of the well-being of the working classes,” as medical historian John Eyler writes in his book “Victorian Social Medicine,”; but also because data were comparatively easy to produce. The emergence of these new societies coincided, in the 1840s, with a wider publishing revolution; new communications and printing technologies were making possible both increasingly affordable and improved-quality print publications, paving the way for early public health visualizations. William Farr, regarded as one of the founders of medical statistics and epidemiology, started his career in medical journalism rather than in practice, which in turn helped him cement his reputation as an expert on vital statistics. In 1839 Farr joined the Statistical Society of London, remaining a core member until his retirement. A regular contributor to one of the world’s oldest medical journals, The Lancet, Farr combined sympathies for liberal reform with the demeanor of the professional statistician. Like many of his peers in the statistical societies of this era, he struggled to balance an ideological inclination toward self-help, with statistical findings that mitigated state intervention. 
The GRO’s policies under Farr were anti-contagionist (in terms of medical outlook), and environmentalist (in terms of reform), writes the late sociologist and historian of science Alain Desrosières. Farr used graphics in his publications for the GRO, some of which, though certainly not innovative, had a striking impact. For example, in his summary report, published in the “Fifth Annual Report” (1843), three line graphs are used to juxtapose mortality rates between Surrey, Liverpool, and an average Metropolis, demonstrating wide variation in the laws of mortality across the distributions. The middle of these three charts, representing Liverpool, showed that half the children there died before the age of 6 — challenging previously held convictions of the time that the rapid growth of the city was proof that its environmental climate was healthy. Another medical journalist who experimented with data visualization, John Snow, started his trade in London during the mid-1830s, having several papers published in The Lancet and the London Medical Gazette. “On the Mode of Transmission of Cholera” (1849) was published in the same year that Snow published articles about cholera in the Medical Gazette and Times. He proposed that the disease was carried in water supplies contaminated with diarrhea and that it passed via human contact and through contact with contaminated matter. 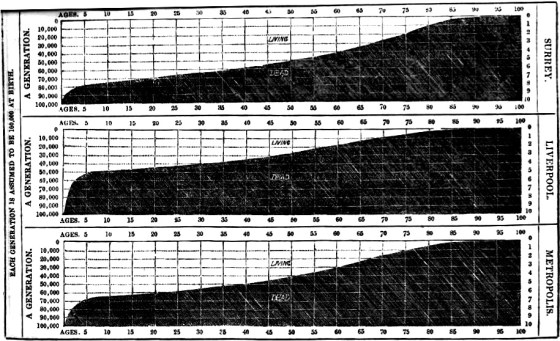
In his statistical maps, he used GRO data reports — “Weekly Return of Births and Deaths in London” — to map local incidences of the disease and to compare them with previous outbreaks. The centrality of Snow’s findings to medical cartography, geography, and epidemiology are long established in the literature — but a question remains as to why he failed to convince his contemporaries of the logical conclusion of his findings. Tom Koch, a clinical ethicist and the author of “Cartographies of Disease,” suggests Snow did not put forward a compelling general theory to substantiate his local findings — he refused to challenge the zymotic theory (the belief that infection was exclusively a consequence of airborne vapors), a theory promoted in the writings, diagrams, and maps of, among others, William Farr. Through family ties, Florence Nightingale, a trailblazing statistician, social reformer, and nursing pioneer, became acquainted with many of the leading medical figures of the day, including Farr. Nightingale and Farr developed a mutually advantageous relationship based on shared goals, at least initially, in which he provided her with statistical advice, while she provided him with access to her politically influential contacts. When the Crimean War broke out in September 1854, The Times’ William Howard Russell sent back a series of damning reports from the front, causing great disquiet among its readers and the wider public, raising awareness of the army’s lack of preparedness, and poor medical management of the wounded. War Secretary Sidney Herbert was compelled to act, asking Nightingale to visit the army hospitals, in the Crimea, at government expense. Just as Nightingale’s presence at Scutari Barracks hospital, Istanbul, had been precipitated by the press, so too her reputation was cultivated, as a consequence of favorable coverage in The Times that popularized her persona as “The Lady with the Lamp” who spent much of her time doting on convalescing soldiers. Although taking up what was primarily an administrative role, Nightingale paid regular visits to the wards, developing a strong affection among the soldiers, leading to her symbolic association with maternal caring. After the war, in September 1856, Nightingale was invited to Balmoral to discuss her experiences and thoughts with Queen Victoria and Prince Albert, leading a few days later to an interview with Lord Panmure, who agreed to the setting up of a commission to investigate the shortcomings of the army’s medical infrastructure. Nightingale’s “Notes on Matters Affecting the Health, Efficiency, and Hospital Administration of the British Army” (1858) was damning in its conclusions about the consequences of the deleterious sanitary conditions in the army hospitals of the Crimea; deaths from (mostly) preventable disease outnumbered deaths on the battlefield (or injuries accrued on the battlefield) by a factor of seven to one. For Nightingale, disease was a quality of the human condition, not something that may be isolated and treated in a particular context. Nightingale had a natural flair for infographic design, or “statistical aesthetics,” to quote John Eyler, which she used to accentuate her work. She was as attuned to the persuasive power of data visualization as she was in her use of written rhetorical techniques. She thought her graphical forms had the power to speak both to the public and to the Queen; however, these forms were not discursively addressed to a wide-ranging, reading public — indeed some were only published, if at all, buried away in the appendixes of several-hundred-page-long government reports. In March 1858, Nightingale developed a sophisticated media campaign, in order to maintain the political momentum of the commission’s findings and to ensure its recommendations were carried out. She identified a number of editors who could be enlisted in getting her message across, supplying their names to the commissioner (and close personal friend) Sydney Herbert. She focused her efforts on the “heavies” — the quarterlies and reviews whose editors garnered a higher degree of respect in polite society than any daily newspaper editor of the day could realistically hope for. Nightingale put together individualized “press packs” for each one of these contacts, comprising “outlines, the facts, even the headings for all articles”; though all were to be published anonymously. Both Nightingale and Farr were concerned in their statistical investigations with uncovering natural laws about human behavior. If man could discover these laws, they reasoned, he might adapt society accordingly, in an act of progressive improvement. This deterministic (albeit not fatalistic) principle owes a debt to Adolphe Quetelet. In 1831, Quetelet published a map of property crimes in France, which was used to visually support his argument that, regardless of human agency, crime obeyed natural laws and increased in relation to increasing social inequality. Quetelet’s approach was empirical, experiential, and predicated on statistical inquiry. Later, his “Sur l’homme et le développement de ses facultés, ou Essai de physique sociale” (1835), the first work to apply statistical method to social problems, exerted a particularly strong influence over Nightingale. In this book she could perceive the intellectual culmination of a mind she thought keenly attuned, like hers, to the systematic collection of data. Nightingale was acutely aware of the rhetorical power of infographics. She took much the same aesthetic delight in statistics as Priestley took in chronographs; they represented for her a “moral imperative, a religious duty,” writes Eyler, toward God’s divinely ordained plan. That said, Nightingale’s contribution to public health was thoroughly pragmatic. She was a shrewd publicist and political actor, but her legacy as a popularizer of infographics is not so clearly established. Those texts containing her diagrams were not commonly available in public library catalogs of the day. Nightingale’s polar area diagrams (or exploded pie charts) owe a debt to William Playfair’s innovations, but also, no doubt, to her long-term collaborator William Farr, who experimented with circular charts in his earlier publications. Lee Brasseur, an expert in the field of visualization, has set out a compelling critique of the visual rhetoric of three of Nightingale’s diagrams as they appear in her 16-page pamphlet, “A Contribution to the Sanitary History of the British Army” (1859) (a publication that attributes tables and diagrams to Farr). These three lithographic prints, published in a short, highly impactful pamphlet, comprise (according to Brasseur) a coherent (and persuasive) sequential progression in visual rhetoric. 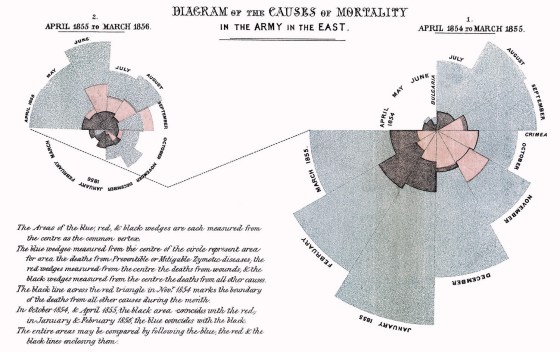
The first, titled “Diagrams of the Mortality in the Army in the East,” sets out monthly mortality rates in the army during the first and second years of the war; the first (larger) diagram concerning mortality rates in the first year draws the viewer’s eye to the right, before a dotted line draws attention over to the smaller diagram on the left, concerning the second year’s mortality rates. The viewer is invited to juxtapose these mortality rates against a concentric circle in each diagram that expresses the average mortality rate of Manchester, one of the deadliest towns in England at the time. Inviting the viewer to reflect upon what might be the cause of these discrepancies, the second chart, “Diagram of the Causes of Mortality in the Army in the East” demonstrates using color-coordinated polar area diagrams that the majority of fatalities are due to preventable disease. Having first set out the scale of the problem, and then second, having explored the reasons for the anomaly, Nightingale then sets out in a third diagram, comprising monthly mortality rates, the outcome of improvements that had been made after March 1855, in Scutari and Kulali army hospitals. Collectively, these three diagrams represent a devastating visual critique of the army’s culpability in many needless deaths at the Crimean front. Nightingale’s polar area diagrams play with the metaphorical implications in William Playfair’s circle diagrams in a highly effective way. These charts challenge the seeming unity, continuity, and coherence of the phenomena they express. The variation in the scaling of each section implies a sense of discontinuity, but also the same spirit of cartographic empiricism that speaks through the wider statistical maps of the 19th century. These forms embolden the viewer with a sense of power, authority, and purpose, to cast a scrutinizing lens over the problem of the social ills of the day. But they also represent discontinuity; things clearly cannot simply go on as they are — change is implicit, change is necessary. This pamphlet is a multimodal medium, combining highly charged interpretive and explanatory discursive elements, into a compelling work of publicity. Nightingale’s approach speaks more to technique than to method. She sought to communicate Quetelet’s foundational statistics to a non-specialist, but nonetheless elite audience. However, passionate statistician though she may have been, the Victorian press had, it seems, little to say about Nightingale’s innovations. Though read within (and presented to) an esteemed audience, the visualizations of Nightingale and Farr could hardly be said to have had a significant, direct public impact. It wouldn’t be until the rise of popular almanacs toward the turn of the 20th century, and in turn the modern daily popular British press, that the wider public would begin to encounter infographics. Murray Dick is a lecturer in multimedia journalism at Newcastle University and the author of “The Infographic: A History of Data Graphics in News and Communications,” from which this article is adapted. from https://ift.tt/2QsW5wg Check out https://takiaisfobia.blogspot.com/ I am behind the wheel of a Nissan Leaf, circling a parking lot, trying not to let the day’s nagging worries and checklists distract me to the point of imperiling pedestrians. Like all drivers, I am unwittingly communicating my stress to this vehicle in countless subtle ways: the strength of my grip on the steering wheel, the slight expansion of my back against the seat as I breathe, the things I mutter to myself as I pilot around cars and distracted pedestrians checking their phones in the parking lot. “Hello, Corinne,” a calm voice says from the audio system. “What’s stressing you out right now?” The conversation that ensues offers a window into the ways in which artificial intelligence could transform our experience behind the wheel: not by driving the car for us, but by taking better care of us as we drive. Before coronavirus drastically altered our routines, three-quarters of U.S. workers--some 118 million people—commuted to the office alone in a car. From 2009 to 2019, Americans added an average of two minutes to their commute each way, according to U.S. Census data. That negligible daily average is driven by a sharp increase in the number of people making “super commutes” of 90 minutes or more each way, a population that increased 32% from 2005 to 2017. The long-term impact of COVID-19 on commuting isn’t clear, but former transit riders who opt to drive instead of crowding into buses or subway cars may well make up for car commuters who skip at least some of their daily drives and work from home instead. Longer commutes are associated with increased physical health risks like high blood pressure, obesity, stroke and sleep disorders. A 2017 research project at the University of the West of England found that every extra minute of the survey respondents’ commutes correlated with lower job and leisure time satisfaction. Adding 20 minutes to a commute, researchers found, has the same depressing effect on job satisfaction as a 19% pay cut. Switching modes of transit can offer some relief: people who walk, bike or take trains to work tend to be happier commuters than those who drive (and, as a University of Amsterdam study recently found, they tend to miss their commute more during lockdown). But reliable public transit is not universally available, nor are decent jobs always close to affordable housing. Technology has long promised that an imminent solution is right around the corner: self-driving cars. In the near future, tech companies claim, humans won’t drive so much as be ferried about by fully autonomous cars that will navigate safely and efficiently to their destinations, leaving the people inside free to sleep, work or relax as easily as if they were on their own couch. A commute might be a lot less stressful if you could nap the whole way there, or get lost in a book or Netflix series without having to worry about exits or collisions. Google executives went on the record claiming self-driving cars would be widely available within five years in 2012; they said the same thing again in 2015. Elon Musk throws out ship dates for fully autonomous Teslas as often as doomsday cult leaders reschedule the end of the world. Yet these forecasted utopias have still not arrived. The majority of carmakers have walked back their most ambitious estimates. It will likely be decades before such cars are a reality for even a majority of drivers. In the meantime, the car commute remains a big, unpleasant, unhacked chunk of time in millions of Americans’ daily lives. A smaller and less heralded group of researchers is working on how cars can make us happier while we drive them. It may be decades before artificial intelligence can completely take over piloting our vehicles. In the short run, however, it may be able to make us happier—and healthier—pilots. Lane changes, left turns, four-way stops and the like are governed by rules, but also rely on drivers’ making on-the-spot judgments with potentially deadly consequences. These are also the moments where driver stress spikes. Many smart car features currently on the market give drivers data that assist with these decisions, like sensors that alert them when cars are in their blind spots or their vehicle is drifting out of its lane. Another thing that causes drivers stress is uncertainty. One 2015 study found commuters who drove themselves to work were more stressed by the journey than were transit riders or other commuters, largely because of the inconsistency that accidents, roadwork and other traffic snarls caused in their schedules. But even if we can’t control the variables that affect a commute, we’re calmer if we can at least anticipate them—hence the popularity of real-time arrival screens at subway and bus stops. The Beaverton, Ore.-based company Traffic Technology Services (TTS) makes a product called the Personal Signal Assistant, a platform that enables cars to communicate with traffic signals in areas where that data is publicly available. TTS’s first client, Audi, used the system to build a tool that counts down the remaining seconds of a red light (visually, on the dashboard) when a car is stopped at one, and suggests speed modifications as the car approaches a green light. The tool was designed to keep traffic flowing—no more honking at distracted drivers who don’t notice the light has turned green. But users also reported a marked decrease in stress. At the moment, the technology works in 26 North American metropolitan areas and two cities in Europe. TTS has 60 full- and part-time employees in the U.S. and Germany, and recently partnered with Lamborghini, Bentley and a handful of corporate clients. Yet CEO Thomas Bauer says it can be hard to interest investors in technologies that focus on improving human drivers’ experience instead of just rendering them obsolete. “We certainly don’t draw the same excitement with investors as [companies focused on] autonomous driving,” Bauer says. “What we do is not quite as exciting because it doesn’t take the driver out of the picture just yet.” Pablo Paredes, an instructor of radiology and psychiatry at the Stanford School of Medicine, is the director of the school’s Pervasive Wellbeing Technology Lab. Situated in a corner of a cavernous Palo Alto, Calif., office building that used to be the headquarters of the defunct health-technology company Theranos, the lab looks for ways to rejigger the habits and objects people use in their everyday lives to improve mental and physical health. Team members don’t have to look far for reminders of what happens when grandiose promises aren’t backed up by data: Theranos’ circular logo is still inlaid in brass in the building’s marble-floored atrium. It can be hard to tell the lab’s experiments from its standard-issue office furniture. To overcome the inertia that often leads users of adjustable-height desks to sit more often than stand, one of the workstations in the team’s cluster of cubicles has been outfitted with a sensor and mechanical nodule that make it rise and lower at preset intervals, smoothly enough that a cup of coffee won’t spill. In early trials, users particularly absorbed in their work just kept typing as the desk rose up and slowly stood along with it. But the millions of hours consumed in the U.S. each day by the daily drive to work hold special fascination for Paredes. He’s drawn to the challenge of transforming a part of the day generally thought of as detrimental to health into something therapeutic. “The commute for me is the big elephant in the room,” he says. “There are very simple things that we’re overlooking in normal life that can be greatly improved and really repurposed to help a lot of people.” In a 2018 study, Paredes and his colleagues found that it’s possible to infer a driver’s muscle tension—a proxy for stress—from the movement of their hands on a car’s steering wheel. They’re now experimenting with cameras that detect neck tension by noting the subtle changes in the angle of a driver’s head as it bobs with the car’s movements. The flagship of the team’s mindful-commuting project is the silver-colored Nissan Leaf in their parking lot. The factory-standard electric vehicle has been tricked out with a suite of technologies designed to work together to decrease a driver’s stress. On a test drive earlier this year, a chatbot speaking through the car’s audio system offered me the option of engaging in a guided breathing exercise. When I verbally agreed, the driver’s seatback began vibrating at intervals, while the voice instructed me to breathe along with its rhythm. The lab published the results of a small study earlier this year showing that the seat-guided exercise reduced driver stress and breathing rates without impairing performance. They are now experimenting with a second vibrating system to see if lower-frequency vibrations could be used to slow breathing rates (and therefore stress) without any conscious effort on the driver’s part. The goal, eventually, is a mass-market car that can detect an elevation in a driver’s stress level, via seat and steering wheel sensors or the neck-tension cameras. It would then automatically engage the calming-breath exercise, or talk through a problem or tell a joke to ease tension, using scripts developed with the input of cognitive behavioral therapists. These technologies have value even as cars’ autonomous capabilities advance, Paredes says. Even if a car is fully self-driving, the human inside will still often be a captive audience of one, encased in a private space with private worries and fears. Smarter technologies alone aren’t the solution to commuters’ problems. The auto industry has a long history of raising drivers’ tolerance for long commutes by making cars more comfortable and attractive places to be—all the while promising a better driving experience that’s just around the corner, says Peter Norton, an associate professor of science, technology, and society at the University of Virginia and author of Fighting Traffic: The Dawn of the Motor Age in the American City. From his perspective, stress-busting seats would join radios and air conditioners as distractions from bigger discussions about planning, transit and growing inequality, all of which could offer much more value to commuters than a nicer car. In addition, how long it will be before these latest features become widely available options is an open question. Paredes’ lab had to suspend work during the pandemic, as it’s hard to maintain social distancing while working inside of a compact sedan. TTS is in talks to expand its offerings to other automakers, and Paredes has filed patents on some of his lab’s inventions. But just because a technology is relatively easy to integrate in a car doesn’t mean it will be standard soon. The first commercially available backup cameras came on the market in 1991. Despite their effectiveness in reducing collisions, only 24% of cars on the road had them by 2016, according to the Insurance Institute for Highway Safety, and most were newer luxury vehicles. (The cameras are now required by law in all new vehicles.) These technologies also raise new questions of inequality and exploitation. It’s one thing for a commuter to opt for a seat that calms them down after a tough day. But if you drive for a living, should the company that owns your vehicle have the right to insist that you use a seat cover that elevates your breath rate and keeps you alert at the wheel? Who owns the health data your car collects, and who gets to access it? All of the unanswered questions that self-driving technologies raise apply to self-soothing technologies as well. Back in Palo Alto, the pandemic still weeks away, I am piloting the Leaf around the parking lot with a member of the lab gamely along for the ride in the back. The chatbot asks again what’s stressing me out. I have a deadline, I say, for a magazine article about cars and artificial intelligence. The bot asks if this problem is “significantly” affecting my life (not really), if I’ve encountered something similar before (yep), if previous strategies could be adapted to this scenario (they can) and when I’ll be able to enter a plan to tackle this problem in my calendar (later, when I’m not driving). I do feel a little better. I talk to myself alone in the car all the time. It’s kind of nice to have the car talk back. “Great. I’m glad you can do something about it. By breaking down a problem into tiny steps, we can often string together a solution,” the car says. “Sound good?” from https://ift.tt/3jfOHAJ Check out https://takiaisfobia.blogspot.com/ Nobody will ever know the identity of the thousands of African children who were not killed or paralyzed by polio this year. They would have been hard to keep track of no matter what because in ordinary times, they would have followed thousands last year and thousands the year before and on back in a generations-long trail of suffering and death. Instead, no African children were claimed by polio this year or last year or the year before. It was in 2016 that the last case of wild, circulating polio was reported in Nigeria—the final country on the 54-nation African continent where the disease was endemic. And with a required multi-year waiting period now having passed with no more cases, the World Health Organization today officially declared the entirety of Africa polio-free. A disease that as recently as the late 1980s was endemic in 125 countries, claiming 350,000 children per year, has now been run to ground in just two remaining places, Pakistan and Afghanistan, where there have been a collective 102 cases so far in 2020. That’s 102 too many, but there is no denying the scope of the WHO announcement. “Today’s victory over the wild poliovirus in the African region is a testament to what can happen when partners from a variety of sectors join forces to accomplish a major global health goal,” says John Hewko, general secretary and CEO of Rotary International. “[It is] something the world can and should aspire to during these turbulent times.” It was Rotary, an international nonprofit service organization, that kicked off the polio endgame in 1988 with the launch of the Global Polio Eradication Initiative (GPEI). That program aimed to leverage the power of Rotary’s 35,000 clubs and 1.22 million members in 200 countries and territories worldwide to make polio only the second human disease—after smallpox—to be pushed over the brink of extinction. The job was made easier by the partners Rotary immediately attracted: the WHO, the U.S. Centers for Disease Control and Prevention (CDC) and UNICEF. The Bill and Melinda Gates Foundation joined in 2007, followed by Gavi, the Vaccine Alliance, just last year. The 32-year initiative has depended on volunteer workers and charitable donations, which together have produced an army of 20 million field workers administering vaccines to over 2.5 billion children at a cost of $17 billion. Some countries were a lighter lift than others. In the U.S. the disease was eradicated in 1979, well before the GPEI even began its work. Other nations followed: In 1994 the Americas were declared polio-free. Europe as a whole got a clean bill of health in 2002, when all 53 countries in the WHO’s designated European region were declared free of the virus. Massive vaccination efforts began in India in 1997, which eradicated the virus in 2014. How Polio Was Eradicated from the African ContinentBut Africa, with its vast sprawl of village populations, long distances to urban hospitals, spotty infrastructure like adequate roads and reliable “cold chains”—refrigerated transport networks to keep vaccines viable—was always going to present special challenges. In 1996, when the case count on the continent regularly reached 75,000 victims every year, South African President Nelson Mandela partnered with Rotary to launch the “Kick Polio Out of Africa” Campaign, and the group scrambled fast—or as fast as was possible with so many children to vaccinate on so vast a land mass. In 2000, the first synchronized campaigns began in 17 countries, with 76 million children being vaccinated by tens of thousands of volunteers. The work fanned out across the continent from there, including an especially heavy push from 2008 to 2010, when an outbreak in 24 countries in western and central Africa was met by a large-scale, multi-national vaccination of 85 million children. Finally, Nigeria stood alone as the only African nation where the disease was still endemic, in part because of resistance by religious leaders in the northern part of the country who objected western interference in local affairs and claimed that the vaccine was unsafe. That opposition broke down, partly thanks to Muhammad Sanusi II, the Emir of the city of Kano—a hereditary leader descended from a ruling family—who appeared at a public ceremony before the kick off of a seasonal vaccination campaign in 2016, called for a vial of polio vaccine to be brought to the stage, and with the audience watching, broke its seal and drank down its entire contents. That year, the country recorded its last case of polio, and this year, Nigeria’s WHO certification is the reward for its efforts. “The polio eradication program in Nigeria has gone through some difficult times, but I never once doubted that this day would come,” says Dr. Tunji Funsho, a former cardiologist who is the chair of Rotary International’s Polio-Plus Committee in Nigeria. “Any time that we’ve experienced a setback, Rotary and our partners have been able to find solutions and develop new strategies for reaching vulnerable children.” The Next Steps Towards Global EradicationOther challenges remain. For one thing there are still the stubborn polio redoubts of Afghanistan and Pakistan, but Funsho is cautiously optimistic. “Afghanistan and Pakistan have their own set of challenges in the fight against the wild poliovirus, but so did the African region and Nigeria,” he says. “I cannot put a time stamp on when wild polio will be eradicated in the two remaining countries. The lessons we’ve learned in Nigeria and the African region show that eradication can only be achieved through global commitment.” What’s more, wild polio is not the only kind that causes disease. The oral vaccine contains a live but weakened virus, which in rare cases can mutate and lead to the very disease it’s designed to prevent. There have been 302 cases of vaccine-derived polio in both endemic and non-endemic countries so far this year—all localized and not widespread like wild polio can be. Again, that case count is small by earlier standards, but again too many by the standards of the children and the families who are its victims. Stopping those infections means eventually supplementing the oral, live-virus vaccine with the injectable variety that uses a killed virus that can never cause the disease. The downside of the killed vaccine: it requires trained health care workers to administer the shots, as opposed to volunteers who can easily learn to place drops in a child’s mouth. That final round of vaccinations will be thus more expensive and labor-intensive than earlier rounds, but only after the handful of vaccine-derived cases are eliminated too, will the scourge of polio at last pass into history. Funsho and others are convinced that will happen. “One thing I know for certain,” he says, “is if Nigeria could eliminate the wild poliovirus, any country can eliminate it.” from https://ift.tt/32lNPE4 Check out https://takiaisfobia.blogspot.com/ Many months into the COVID-19 pandemic, the coronavirus is still spreading uncontrolled through the U.S. Public health authorities including the U.S. Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) tell us to remain six feet apart, wash our hands, disinfect frequently touched surfaces, and wear masks. But compliance with these measures—especially masks—is mixed, and daily we hear of cases where people do not know how they were infected. We hear about superspreading events, where one person infects many, happening in crowded bars and family gatherings, but not at outdoor demonstrations. Beaches in cities like Chicago are closed, but gyms and indoor dining at restaurants have reopened. It is no wonder the public is confused. It is critical to have a clear physical description of the ways in which COVID-19 is transmitted, so that individuals and institutions are able to visualize it and will understand how to protect themselves. Contrary to public health messaging, I, together with many other scientists, believe that a substantial share of COVID-19 cases are the result of transmission through aerosols. The evidence in favor of aerosols is stronger than that for any other pathway, and officials need to be more aggressive in expressing this reality if we want to get the pandemic under control. There are three possible ways the virus is transmitted, of which two have been emphasized by the WHO and the CDC. The first is through “fomites,” objects that are contaminated with the virus (which could include someone else’s skin). Early in the pandemic, concern over fomite transmission drove some people to bleach groceries and packages. The CDC now says fomites are a possible means of transmission, but likely not one that is major. For example, an intensive handwashing program in the UK led to only a 16% reduction in transmission. Significantly, other viruses that, like SARS-CoV-2 (the one that causes COVID-19), have a lipid envelope, do not survive long on human hands. That means someone would need to touch their eyes, nostrils, or mouth a short time after touching a contaminated surface in order to contract the novel coronavirus. The second possibility for how COVID-19 spreads is through droplets, small bits of saliva or respiratory fluid that infected individuals expel when they cough, sneeze, or talk. Droplets—which the WHO and CDC maintain is the primary means of transmission of COVID-19—are propelled through the air, but fall to the ground after traveling 3-6 feet. However, published research, which has been replicated, shows that droplets are only important when coughing and sneezing. But when it comes to talking in close proximity, which appears to play a major role in COVID-19 transmission, droplets are less important than the third potential pathway: aerosols. Many diseases, including COVID-19, infect most effectively at close proximity. Since droplets are visible and fall to the ground between 3-6 feet, we can readily see and understand this route of infection. In fact, it was thought for decades that tuberculosis was transmitted by droplets and fomites, based on ease of infection at close proximity, but research eventually proved that tuberculosis can only be transmitted through aerosols. I believe that we have been making a similar mistake for COVID-19. “Aerosol” (sometimes referred to as “airborne”) transmission is similar to droplet transmission, except that the bits of fluid are so small that they can linger in the air for minutes to hours. To understand the scale of aerosols, the diameter of a human hair is about 80 microns, and aerosols smaller than about 50 microns can float in the air long enough to be inhaled. SARS-CoV-2 is only 0.1 microns in diameter, so there is room for plenty of viruses in aerosols. Fomites and droplets have dominated our everyday understanding of COVID-19 transmission. While the WHO and CDC both state that aerosols could lead to transmission under highly specific situations, both organizations maintain that they are less important. I believe this is a significant mistake and on July 6 I, along with 239 scientists, appealed to the WHO to reevaluate their stance. WHO updated its position in response, but the agency’s language continues to express skepticism of the importance of this pathway. The unwillingness to acknowledge the likelihood that aerosols are a major means of COVID-19 transmission can be traced to the legacy of Dr. Charles Chapin, an American public health researcher. Trying to bury once and for all the theory of miasmas, ghostly clouds of disease, he argued in his seminal 1910 book The Sources and Modes of Infection that aerosol transmission was nearly impossible. “It will be a great relief to most persons to be freed from the specter of infected air, a specter that has pursued the race since the time of Hippocrates,” Chapin wrote. The impact of his book was fortuitous in a way: it came at a time when enough evidence about the transmission of different infectious diseases had accumulated since the discovery of germs by Pasteur in the 1860s, but before we had the technology to measure aerosols. Chapin’s notions became the paradigm of infectious disease transmission, which has dominated until now. Given this deeply held disbelief of aerosol transmission, just a few diseases, including measles and chickenpox, have been accepted as being transmitted through aerosols—and only because these are so transmissible that the evidence could not be ignored by the medical community. Some less-contagious respiratory diseases, like influenza, were described as due to droplet and fomite transmission, even when they clearly had an aerosol component. That stance has, over the years, created an unfounded perception in health care that any disease that is transmitted through aerosols has to be extremely contagious. But 110 years later, the nuances and importance of aerosol transmission of respiratory diseases are finally becoming mainstream. When it comes to COVID-19, the evidence overwhelmingly supports aerosol transmission, and there are no strong arguments against it. For example, contact tracing has found that much COVID-19 transmission occurs in close proximity, but that many people who share the same home with an infected person do not get the disease. To understand why, it is useful to use cigarette or vaping smoke (which is also an aerosol) as an analog. Imagine sharing a home with a smoker: if you stood close to the smoker while talking, you would inhale a great deal of smoke. Replace the smoke with virus-containing aerosols, which behave very similarly, and the impact is similar: the closer you are to someone releasing virus-carrying aerosols, the more likely you are to breathe in larger amounts of virus. We know from detailed, rigorous studies that when individuals talk in close proximity, aerosols dominate transmission and droplets are nearly negligible. If you are standing on the other side of the room, you would inhale significantly less smoke. But in a poorly ventilated room, the smoke will accumulate, and people in the room may end up inhaling a lot of smoke over time. Talking, and especially singing and shouting increase aerosol exhalation by factors of 10 and 50, respectively. Indeed, we are finding that outbreaks often occur when people gather in crowded, insufficiently ventilated indoor spaces, such as singing at karaoke parties, cheering at clubs, having conversations in bars, and exercising in gyms. Superspreading events, where one person infects many, occur almost exclusively in indoor locations and are driving the pandemic. These observations are easily explained by aerosols, and are very difficult or impossible to explain by droplets or fomites. Furthermore, droplets move ballistically—they fly like a cannonball from someone’s mouth and then travel through the air until they either hit something (worst case someone else’s eyes, mouth or nostrils) or fall to the ground. Aerosols on the other hand, act like smoke: after being expelled, they don’t fall to the ground, but rather disperse throughout the air, getting diluted by air currents, and being inhaled by others present in the same space. Contact tracing shows that, when it comes to COVID-19, being outdoors is 20 times safer than being indoors, which argues that aerosol transmission is much more important than droplets; outdoors, there’s plenty of air in which aerosols can become diluted; not so indoors. In addition, researchers have demonstrated aerosol transmission of this virus in ferrets and hamsters. The visual analogy of smoke can help guide our risk assessment and risk reduction strategies. One just has to imagine that others they encounter are all smoking, and the goal is to breathe as little smoke as possible. But COVID-19 is not very contagious under most situations, unlike, for example, measles: the CDC says that 15 minutes of close proximity to a COVID-19 infected person often leads to contagion, which provides an estimate of how much “exhaled smoke” one may need to inhale for infection. Inhaling a little whiff of “smoke” here and there is OK, but a lot of “smoke” for a sustained period of time and without a mask is risky. (To be clear, actual smoke does not increase the probability of infection.) We should continue doing what has already been recommended: wash hands, keep six feet apart, and so on. But that is not enough. A new, consistent and logical set of recommendations must emerge to reduce aerosol transmission. I propose the following: Avoid Crowding, Indoors, low Ventilation, Close proximity, long Duration, Unmasked, Talking/singing/Yelling (“A CIViC DUTY”). These are the important factors in mathematical models of aerosol transmission, and can also be simply understood as factors that impact how much “smoke” we would inhale. A CIViC DUTY first suggests that we should do as many activities as possible outdoors, as schools did to avoid the spread of tuberculosis a century ago, despite harsh winters. Given how much being outside reduces COVID-19 transmission risk, it is mind boggling that the U.S. National Guard is not busy setting up open canopy tents at every school around the country. That said, stepping outdoors is not a magical protection against contagion: a windy day in an open area while keeping our distance is very safe, but an unmasked close conversation with still air in a narrow passage between tall buildings is risky. Second, masks are essential, even when we are able to maintain social distance. We should also pay attention to fitting masks snugly, as they are not just a parapet against ballistic droplets, but also a means to prevent “smoke” from leaking in through gaps. We should not remove masks to talk, nor allow someone who is not wearing a mask to talk to us, because we exhale aerosols 10 times as much when talking compared to breathing. Everyone should be careful to not stand behind someone with a poorly fitting mask, as the curvature of an ill-fitting mask can cause aerosols to travel behind the person wearing it. It is important to think about ventilation and air cleaning. We take operable windows and HVAC systems for granted, rarely paying attention to how they work. Times are different now, and we need to learn how to best use these systems to decrease risk. We need to increase the amount of indoor air that is replaced by outdoor air, by opening windows or adjusting mechanical systems. We need better filters installed in many ventilation systems that recirculate some of the air. These interventions can get costly, so it is very important to think carefully and prioritize objectively—we can, for example, use affordable CO2 measurements to identify the most dangerous, underventilated frequently occupied public spaces, and prioritize them. Portable HEPA air cleaners work well to remove virus-laden aerosols, but unfortunately they are costly. Makeshift fan-filter cleaners can be made for less than $50, have been shown to work in multiple tests including peer-reviewed papers, and have been used for years in China to reduce the impact of pollution in homes. They can be noisy and are not a long-term solution, but they may help us get through the next few months. Germicidal UV systems can help in some situations, but only if ventilation and filtering cannot do the job. We should also remember that air cleaning is not a silver bullet: if we simulate the Skagit choir outbreak with an added large amount of air cleaning, the infection rate only drops by half. Spending as much time as possible outdoors, wearing masks, and reducing density will remain critical no matter how well we ventilate and clean the air. In a fast-moving viral pandemic, scientific understanding will inevitably change as research catches up to the speed at which the virus spreads. However, it seems clear that aerosols are more important when it comes to transmitting COVID-19 than we thought six months ago—and certainly more important than public health officials are currently making them out to be. The WHO and CDC, among others, must begin communicating the science suggesting aerosol spread of COVID-19—and the risk reduction strategies necessary as a result. If not, we hamper our ability to counter the growing health consequences and increasing death toll of COVID-19. from https://ift.tt/2QjvrGe Check out https://takiaisfobia.blogspot.com/ Over the past few years, Professor Zhang Yongzhen has made it his business to sequence thousands of previously unknown viruses. But he knew straight away that this one was particularly nasty. It was about 1:30 p.m. on Jan. 3 that a metal box arrived at the drab, beige buildings that house the Shanghai Public Health Clinical Center. Inside was a test tube packed in dry ice that contained swabs from a patient suffering from a peculiar pneumonia sweeping China’s central city of Wuhan. But little did Zhang know that that box would also unleash a vicious squall of blame and geopolitical acrimony worthy of Pandora herself. Now, he is seeking to set the record straight. Zhang and his team set to work, analyzing the samples using the latest high-throughput sequencing technology for RNA, the viral genetic building blocks, which function similar to how DNA works in humans. By 2 a.m. on Jan. 5, after toiling through two nights straight, they had mapped the first complete genome of the virus that has now sickened 23 million and killed 810,000 across the globe: SARS-CoV-2. “It took us less than 40 hours, so very, very fast,” Zhang tells TIME in an exclusive interview. “Then I realized that this virus is closely related to SARS, probably 80%. So certainly, it was very dangerous.” The events that followed Zhang’s discovery have since become swathed in controversy. Crises beget scapegoats and the coronavirus is no different. The floundering U.S. response to the pandemic has prompted a wave of racially tinged soundbites, such as “China virus” and “Kung Flu,” as President Donald Trump’s Administration seeks to divert blame onto the nation where the pathogen was first identified. “The outbreak of COVID angered many people in the Administration and presented an election issue for President Trump,” Ambassador Jeffrey Bader, formerly President Obama’s chief adviser on Asia, said at a recent meeting of the Foreign Correspondents Club of China. Read more: Inside the Global Quest to Trace the Origins of COVID-19—and Predict Where It Will Go Next Upon first obtaining the genome, Zhang says he immediately called Dr. Zhao Su, head of respiratory medicine at Wuhan Central Hospital, to request the clinical data of the relevant patient. “I couldn’t say it was more dangerous than SARS, but I told him it was certainly more dangerous than influenza or Avian flu H5N1,” says Zhang. He then contacted China’s Ministry of Health and traveled to Wuhan, where he spoke to top public health officials over dinner Jan. 8. “I had two judgements: first that it was a SARS-like virus; second, that the virus transmits by the respiratory tract. And so, I had two suggestions: that we should take some emergency public measures to protect against this disease; also, clinics should develop antiviral treatments.” Afterward, Zhang returned to Shanghai and prepared to travel to Beijing for more meetings. On the morning of Jan. 11, he was on the runway at Shanghai Hongqiao Airport when he received a phone call from a colleague, Professor Edward Holmes at the University of Sydney. A few minutes later, Zhang was strapped in for takeoff and still on the phone—then Holmes asked permission to release the genome publicly. “I asked Eddie to give me one minute to think,’” Zhang recalls. “Then I said ok.” For the next two hours, Zhang was cocooned from the world at 35,000 feet, but Holmes’ post on the website Virological.org sent shockwaves through the global scientific community. By the time Zhang touched down in Beijing, his discovery was headline news. Officials swooped on his laboratory to demand an explanation. “Maybe they couldn’t understand how we obtained the genome sequence so fast,” says Zhang. “Maybe they didn’t fully believe our genome. So, I think it’s normal for the authorities to check our lab, our protocols.” Read more: China Says It’s Beating Coronavirus. But Can We Believe Its Numbers? Critics of China’s response have latched onto the Jan. 11 date of publication as evidence of a cover-up: why, they ask, didn’t Zhang publish it on Jan. 5, when he first finished the sequencing? Also, Zhang’s lab was probed by Chinese authorities for “rectification,” an obscure term to imply some malfeasance. To many observers, it seemed that furious officials scrambling to snuff out evidence of the outbreak were punishing Zhang simply for sharing the SARS-CoV-2 genome—and in the meanwhile, slowing down the release of this key information. Yet Zhang denies reports in Western media that his laboratory suffered any prolonged closure, and instead says it was working furiously during the early days of the outbreak. “From late January to April, we screened more than 30,000 viral samples,” says Fan Wu, a researcher who assisted Zhang with the first SARS-CoV-2 sequencing. And, in fact, Zhang insists he first uploaded the genome to the U.S. National Center for Biotechnology Information (NCBI) on Jan. 5—an assertion corroborated by the submission date listed on the U.S government institution’s Genbank. “When we posted the genome on Jan. 5, the United States certainly knew about this virus,” he says. But it can take days or even weeks for the NCBI to look at a submission, and given the gravity of the situation and buoyed by the urging of colleagues, Zhang chose to expedite its release to the public, by publishing it online. (Approached by TIME, Holmes deferred to Zhang’s version of events.) It’s a decision that facilitated the swift development of testing kits, as well as the early discussion of antivirals and possible vaccines. Zhang, 55, is keen to downplay the bravery of his actions. But the stakes of doing what is right over what one is told are rendered far higher in authoritarian systems like China’s. Several whistleblower doctors were detained early in the pandemic. According to a Jan. 3 order seen by respected Beijing-based finance magazine Caixin, China’s National Health Commission, the nation’s top health authority, forbade the publishing of any information regarding the Wuhan disease, while labs were told to destroy or transfer all viral samples to designated testing institutions. Caixin also reports that other labs had processed genome sequences before Zhang obtained his sample. None were published. It’s difficult to know what conclusions to draw. Dr. Dale Fisher, head of infectious diseases at Singapore’s National University Hospital, says he doesn’t think that any delay by the Chinese authorities was malicious. “It was more like appropriate verification,” he says. Fisher traveled to China as part of a World Health Organization (WHO) delegation in early February and says outbreak settings are always confusing and chaotic with people unsure what to believe. “To actually have the whole genome sequence by early January was outstanding compared to outbreaks of the past.” Of course, Zhang’s fears based on the viral genome were just one evidence strut to inform China’s decision-making process, alongside public health data and clinical reports about specific cases. Despite mounting evidence of human-to-human transmission, including doctors falling ill, it was only on Jan. 20 that China officially confirmed community transmission. Two days later, Wuhan’s 11 million residents were placed on a bruising lockdown that would last for 76 days. Even while the WHO publicly praised China for transparency, internal documents seen by the Associated Press suggest health officials were privately frustrated by the slow release of information. One joint study by scientists in China, the U.K. and U.S. suggests there would have been 95% fewer cases in China had lockdown measures been introduced three weeks earlier. Two weeks earlier, 86% fewer; one week, 66% fewer. Yet there was some historical basis for skepticism about the severity of the emerging viral disease. After all, the last global pandemic—the swine flu outbreak of 2009—was far less deadly than initially feared, mainly because many older people had some immunity to the virus, leading to criticism that the WHO was overly hasty and even overly dramatic in declaring a pandemic when the virology didn’t warrant it. “In China, even though we had a very bad experience with SARS and other diseases, in the beginning nobody—not even experts from China’s CDC and the Ministry of Health—predicted the disease could be quite so bad,” says Zhang. Donald Trump disagrees. He has repeatedly claimed that swifter action by China could have stopped the pandemic in its tracks. “The virus came from China,” Trump said Aug. 10. “It’s China’s fault.” Beijing concedes that mistakes were made at the outset, though insists that blame lies solely with bungling local officials (who have since been punished for those failures), while the central government’s response was exemplary. This is, of course, its own politically motivated oversimplification. On both sides, wild accusations have eclipsed reason as Sino-U.S. relations spiral to an unprecedented nadir. While U.S. officials have suggested that COVD-19 originated in a Wuhan laboratory, their Chinese counterparts have propagated conspiracy theories that the U.S. military is responsible. “It’s not a good thing for China and the U.S. to be involved in this struggle,” says Zhang. “If we can’t work together, we can’t solve anything.” Read more: The Coronavirus Outbreak Could Derail Xi Jinping’s Dreams of a Chinese Century Some facts are undeniable. The first U.S. case was confirmed on Jan. 21—a man in his 30s who had just returned from Wuhan to his hometown in Washington State. Japan confirmed its first coronavirus case one day later, and reported the world’s highest infection number early in the outbreak, before getting a handle on the situation. Today, the U.S. has 16,407 cases per million population compared with 462 in Japan. Across the world, authoritarian and democratic nations have both handled the crisis well and poorly. For its part, the global scientific community has risen to the challenge, working across national boundaries to advance understanding of the disease, including priceless collaborations between Chinese and Western virologists. Previously, the best described epidemic in terms of viral genetics was the 2014 West African Ebola outbreak. Then, about 1,600 genomes were mapped over three years, providing insights into how viruses move between locations and accumulate genetic differences as they do. But for SARS-CoV-2, following Zhang’s initial genome, scientists mapped about 20,000 within three months. Genomic surveillance enables scientists to trace the speed and character of genetic changes, with ramifications for infection rates and the production of vaccines and antivirals. “Very large-scale genomic screening can evaluate whether any resistance mutations have occurred and, if they do, how those spread through time,” says Oliver Prybus, professor of evolution and infectious disease at Oxford University. For Zhang, focus must now be on understanding how pathogens and the environment interact. Over the past century, an inordinate number of new viral diseases have emerged in China, including the 1956 Asian Flu, 2002 SARS and 2013 H7N9. Zhang attributes this to China’s diverse ecology and enormous population. Moreover, as China’s economy boomed its people have begun traveling far and wide in search of work, education and opportunities. According to the World Bank, almost 200 million people moved to urban areas in East Asia during the first decade of the 21st century. In China, 61% of the population lived in urban areas in 2020 compared with just 18% in 1978. This brings unknown pathogens and people without natural defenses into close proximity. “People and pathogens must be in contact [for outbreaks],” says Zhang. “If no contact, no disease.” As urbanization intensifies, outbreaks of pathogenic diseases will only become more common. Mitigation, says Zhang, comes from deeper understanding of viruses, so that we can accurately map and predict which are likely to spill over into human populations. Just as satellites have made forecasting weather patterns unerringly reliable, Zhang believes science holds the key to predicting viral outbreaks with similar accuracy as with which we now anticipate typhoons and tornadoes. “If we don’t learn lessons from this disease,” says Zhang, “humankind will suffer another.” from https://ift.tt/34xUlKq Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
