|
<strong>You are the sky. </strong></p> <p class="quoteText" style="text-align: center;"><strong>Everything else – it’s just the weather.</strong> A slew of beloved friends have been having babies lately. I’m embarrassingly emotional about their arrival, or even just the news that they’re on their way. Knowing that this new crop of young ones will uncover delight in this bruised world just as children always have is sustaining right now. It’s been a fractious and scary year, but these pandemic babies will still laugh deliriously at the smallest of forgotten joys, like squeezing mashed potatoes through their fingers or grabbing the dog’s nose. And in turn, that’ll make the adults who love them crack up. It’s an ordinary but precious intergenerational symphony. We believe our job is to teach kids everything, meanwhile, they’re reminding us how to be alive and present. I like thinking that this newest generation will be better than we are, maybe because they are such a stubbornly optimistic bet on the future in the face of what economists predict will be a drop in birth rates for 2021. This delay in parenthood is the price of economic hardship, a pandemic, and political agonies across the globe. Surely this baby bust will wane as we emerge into the light of what looks like it will be a summer of optimism. However, the idea that so many people may have already put off having babies for financial reasons or because they’ve borne the brunt of the pandemic childcare nightmare is logical and will have its own aftershock. Women, in particular, have spent the last 15 months stretching themselves to the breaking point to fill the massive gaps in our care economy during this long crisis, whether it’s working and homeschooling kids or taking care of elderly relatives, and often all three. This saga reminds me of how my sister and I waited to have kids like many in our cohort, and the story I wrote about that calculus of care–can your parents be the babysitters or will they need care themselves? After this year, and its toll on seniors, the latter is more likely. 
A few years ago I was sitting in the vast dining room of an assisted-living home in Washington, D.C., watching my then-5-year-old niece bounce like a pinball between tables of seniors. It was a startling sight–that small, bright-eyed blur amid a hundred crinkly faces. Her audience, mostly women in their 80s and 90s, grinned as she navigated all the parked walkers, canes, and wheelchairs as if it were a playground. Sahar was a bit of a celebrity at the residence. Far younger than most of the other grandchildren who visit, she was a rare burst of kindergarten energy in a place where even the elevators move very slowly. She came frequently to have meals with my dad, her grandfather. He was 81, and she didn’t know what he was like before dementia took hold. Nor does she remember her grandmother who died several years ago, except in the funny stories my sister tells so often that Sahar refers to them as if they were her own memories. These Gen Z kids have seen us juggle our jobs, their school schedules and their grandparents’ needs simultaneously–one day missing work to be at the bedside of a parent who’s had a bad fall, another day trying to call an elder-care aide from the back row of a dance recital.Sahar and my two children are among a growing number of kids who will see their grandparents primarily as people in need of care rather than as caretakers. They are the leading edge of a generation whose mothers and fathers had children later in life. It seems naive to say this tripart balancing act came as a surprise to me and my sister, but it did. Somehow, while we were worrying about our biological clocks and our careers, it didn’t occur to us that another biological clock was ticking down: that of our parents’ health. And although medical science keeps coming up with new ways to prolong fertility, thwarting the frailties of old age is harder. Our parents seemed so vibrant, so capable in their 60s that we couldn’t imagine how fast things would change. We knew that three or four years could make a huge difference in our fertility, but it turned out that three or four years could also mean the difference between a grandmother who can take a toddler to the beach and one who can’t lift her newest grandbaby out of a kiddie pool because of arthritis. Did someone forward you this newsletter? Subscribe here to get a weekly essay. My children may face an even greater grandparent gap. I was almost 39 when I had my second child. If she has a child at the same age, I’ll be over 80 when that grandchild enters pre-K. And I’m not alone here: about six times as many children were born to women 35 and older in 2012 as they were 40 years ago. I’m aiming to stay spry, but by the time I become a grandmother, I’ll likely be past the age that my daughter can drop her kids off at my house for a weekend. Will I be one of those exceptional octogenarians who jogs every day? Will I be able to babysit, or will I need my daughter to find me a babysitter? I don’t know. But with about half a million people diagnosed with Alzheimer’s each year, plus the usual maladies of age, there’s a fair chance I’ll need some kind of help. If I had thought about all that, I might have gotten pregnant a few years earlier, just to give my kids that little bit of extra time with my parents in their prime. Of course, it’s not as if my sister and I could have chosen exactly when we met the men who became our children’s fathers. Nor do I regret spending my 20s and part of my 30s living in different countries, doing all kinds of jobs, soaking up the world. It was glorious, and it made me a better mother. But I do know I’d give anything if my kids could have one more weekend at the beach with my parents in peak grandparenting mode–full of dumb puns and poetry and wry observations from the extraordinary lives they’d lived so fully. And now, amid the ongoing debate over when to lean into a job or a relationship or children, my take has changed. I want to tell my kids, “Don’t forget the benefits of grandparents in the high-pressure calculus of modern life. I would like to make it easier for you if you want to lean in and have babies at the same time. I’d also like to know your children.” Who knows if I’ll get that chance, given the million variables at play, but I want them to know it’s an option. With my father’s illness, my children discovered that they are not always the center of the world, and they learned to care for him which is a too-rare lesson. And while my young niece (pictured between my dad and my youngest daughter above) never knew what my dad was like when he used to hide Easter eggs or swim after us pretending to be a shark, his white hair pluming like sea foam, she’s learning something beautiful from her mother. She saw my sister visiting him daily, feeding him, talking to him. Sahar saw kindness firsthand. And believe that she understood that the thin, confused man in the bed was someone worth loving. That he was family. New to It’s Not Just You? Subscribe here to get a fresh edition of the newsletter every Sunday. ROAD TRIP ALERT ?Dog and I are departing for that long-awaited cross-country road trip with our friends on May 30th. I’ll be posting updates on Instagram @SusannaSchrobs. 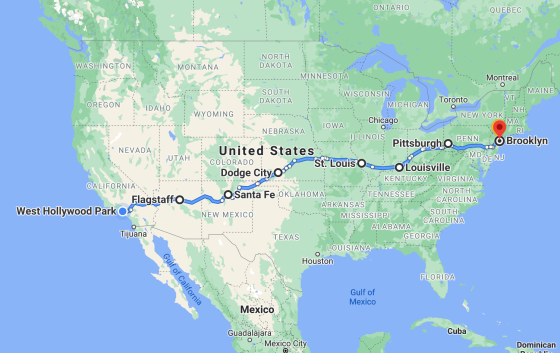
P.S. if you have breakfast restaurant recommendations for any of these cities, DM me, or email me at [email protected] with comments. EVIDENCE OF HUMAN KINDNESS❤️Here’s your weekly reminder that creating a community of generosity elevates us all. 
A LOVE TRANSPLANTEnam and Carlin Jordan, parents of three boys in North Carolina spend $2,000 to $3,000 per month on treatments for two-year-old ‘Baby Carlin’ who was born with sickle cell anemia, a blood disorder that disproportionately affects African Americans. The Jordans, both of whom are youth pastors, are featured in an upcoming episode of Going From Broke, a streaming program that provides financial advice and strategies to those struggling with student loan debt. But because it was impossible for the family to manage their loans along with the burden of their son’s treatments, the show’s producers contacted Pandemic of Love, a grassroots mutual aid organization for help. The only known cure for sickle cell disease is a blood stem cell or bone marrow transplant from a genetically matched donor. Carlin and Enam’s youngest son, six-month-old Caiden, is a match and could be a donor for his big brother, but the cost of this procedure is a staggering $40,000. Enter Pandemic of Love. The group’s volunteers and donors were able to raise the funds needed to underwrite the cost of a bone marrow transplant which was not covered by the couple’s insurance. Check out this emotional video clip in which Enam and Carlin were surprised with a check for their son’s transplant. The pair were moved to tears saying: “Words cannot describe how blessed our family has been by this generous and selfless donation.” (See the full episode about the Jordans in season two of Going From Broke.) Story and images courtesy of Shelly Tygielski, founder of Pandemic of Love, a grassroots organization that matches volunteers, donors, and those in need. COMFORT CREATURESOur weekly acknowledgment of the animals that help us make it through the storm. This is Spring, submitted by Melanie who writes: “This is my son’s first puppy and my first in over 17 years. She has brought so much love, joy, and chaos into our life.” (Send your comfort creature images with captions to: [email protected]) 
Share this edition of It’s Not Just You here. Did someone forward you this newsletter? SUBSCRIBE to It’s Not Just You here. from https://ift.tt/3fA0088 Check out https://takiaisfobia.blogspot.com/
0 Comments
In a recent Morbidity and Mortality Weekly Report (MMWR), researchers at the U.S. Centers for Disease Control (CDC) provide the first wide-scale look at the number of so-called “breakthrough infections”—COVID-19 infections occurring in people who are vaccinated against the disease. Among more than 101 million people who were fully vaccinated in the U.S. during the study period from Jan. to April 30—meaning they were two weeks out from their last vaccine dose—10,262 cases of SARS-CoV-2 infection were reported by state and local health departments to the CDC. That works out to just 0.01% of vaccinated people with a confirmed infection, an “incredibly low rate,” says Dr. Carlos del Rio, professor of medicine in the division of infectious diseases at Emory University. “To me, this is just reassuring evidence that vaccines really work.” No vaccine is 100% effective in protecting people from infection. And indeed, the three vaccines currently authorized in the U.S.—from Pfizer-BioNTech, Moderna and Johnson&Johnson-Janssen—were authorized on the basis of their ability to protect people against symptoms of COVID-19, not infection. But in the months since the vaccines rolled out, scientists have documented that people who are vaccinated have lower rates of infection than those who are unvaccinated. In a previous MMWR, published in March, the CDC reported that in a study of nearly 4,000 health care workers, the two mRNA vaccines made by Pfizer-BioNTech and Moderna, were 90% effective in protecting people from getting infected with SARS-CoV-2. And that protection is confirmed in a far larger population of people by the current report. About 27% of the breakthrough infections among the 101 million people vaccinated occurred among those who experienced no symptoms of COVID-19, about 10%, or 995 cases, were known to be hospitalized, and 2%, or 160 people, died. And among those who were hospitalized, nearly a third were hospitalized for something other than COVID-19, and among those that died, about a fifth died of something other than COVID-19. “At the end of the day, I think this is very good news,” says del Rio. “And when breakthrough infections do occur, in general they don’t have serious clinical consequences. So I think in general this is incredibly reassuring.” Dr. Bonnie Maldonado, professor of pediatrics, epidemiology and population health at Stanford University and a member of the CDC committee that reviews vaccines and comes up with immunization recommendations, agrees. “Frankly I think the numbers are amazing. These are miracle vaccines, with better than 90% efficacy in clinical trials, a 0.01% breakthrough infection rate, and almost no severe illness out of 100 million people tracked. It’s about the best information I could expect,” she says. The CDC data also explored to a limited extent what role new variants of SARS-CoV-2, which spread more easily among people and can cause more severe illness, played in the breakthrough infections. Researchers genetically sequenced the virus from only about 5% of the breakthrough infection cases, however, so the data aren’t robust. But so far, it shows that slightly more than half of the infections could be traced to the most common variant, B.1.1.7 (the one first identified in the U.K.), with a recently identified variant from California contributing to about a quarter of the infections. But since overall the percentage of breakthrough infections is small, the immunity produced by the vaccines still appears to be sufficient at protecting against infection with these variants, and, if infections do occur, they lead to less severe disease in many cases. The authors note that the infections reported could be an underestimate of actual breakthrough infections, since the reporting is voluntary, and because many people who are positive may not feel symptoms and therefore would not get tested and diagnosed. Still, based on experience with other vaccines, public health experts expect that the rate will remain low, given how effective the COVID-19 vaccines are in producing antibodies that neutralize the virus as well as longer lasting immune defenses. As a result of these new data, the CDC has told states and local health departments they no longer need to report all cases of breakthrough infections, and instead to just notify CDC when these cases result in hospitalization, severe disease or death. “These [cases] are the ones we’re most concerned about,” CDC director Dr. Rochelle Walensky said during a press briefing addressing the change. Maldonado says there isn’t much added value in continuing to ask for all breakthrough infections, particularly since so many appear to occur without any symptoms. The breakthrough cases resulting in hospitalization or death will, she says, serve as a canary in the coal mine for when vaccine protection might be waning for whatever reason. That could, potentially, simply happen as a result of time passing. “By the end of this year, most of the early people will have been vaccinated about a year, and we might have to rethink then what gets reported and what doesn’t get reported,” says Maldonado. “Because then the question is, will we start losing immunity a year out?” She says state and local health departments will continue tracking all new COVID-19 cases—just not reporting the milder ones to the CDC. If cases start going up, then health experts can investigate the data to see if it looks like vaccinated people are starting to get infected more, and if so, whether variants might be responsible. For now, says Maldonado, the concern should be about people who aren’t vaccinated. That’s where new infections are starting and spreading to cause the breakthrough cases. “The vaccine is 0% effective if you don’t get it,” she says.
from https://ift.tt/2RRPKPo Check out https://takiaisfobia.blogspot.com/ (COLUMBUS, Ohio) — The first winner of Ohio’s first $1 million Vax-a-Million vaccination incentive prize was driving to her family’s home in suburban Cleveland when she received a call about the good news — from Gov. Mike DeWine. A few minutes later Abbigail Bugenske was in her parents’ house screaming so loudly they thought she was crying. “A whirlwind,” Bugenske, 22, said Thursday morning during a news conference. “It absolutely has not processed yet. I am still digesting it — and I like to say that it feels like this is happening to a different person. I cannot believe it.” Bugenske is a mechanical engineer working for GE Aviation in suburban Cincinnati, and has no plans to quit her job. She grew up in Shaker Heights near Cleveland and is a 2020 graduate of Michigan State University. She said she plans to donate to charities but then invest most of it. She was on her way to Cleveland to look at used cars when she got the word, she said, and added: “I think buying a used car is still in my future.” The winner of a full college scholarship was eighth grader Joseph Costello of Englewood near Dayton. “Very excited,” Costello said as he sat between his parents, Colleen and Rich, during the virtual news conference. Although it’s a long way off, Joseph said he’s thought about Ohio State or Miami of Ohio for college. Colleen Costello said she got the call from the governor as she left work Wednesday. At first she thought it was a recording, then realized it was DeWine himself. “I was really thankful at that moment that there was a bench nearby, because I needed to sit down,” she said. DeWine visited with the Costello family in person along with his wife, Fran DeWine, on Wednesday, after the announcement. He said he didn’t know the names of the winners until shortly before he made the calls. “Calling someone and telling them that they’ve won million dollars is a great thing, and calling a family and telling them that they have a scholarship paid for four years is also fun,” the governor said. Bugenske said she received the Moderna vaccine as soon as she was eligible, long before the lottery was announced. The Costellos said they were already vaccinated and had planned to have their children vaccinated by the end of the month, but the lottery announcement inspired them to move those appointments up. During a scheduled visit to Cleveland Thursday, President Joe Biden said, “Ohio has a new millionaire! I tell you what, who wouldathunk it, a million bucks for getting a vaccine? But it’s working.” More than 2.7 million adults signed up for the $1 million prize and more than 104,000 children ages 12 to 17 entered the drawing for the college scholarship, which includes tuition, room and board, and books. Four more $1 million and college scholarship winners will be announced each Wednesday for the next four weeks. DeWine, a Republican, announced the program May 12 to boost lagging vaccination rates. The Ohio Lottery conducted the first drawing Monday afternoon at its draw studio in Cleveland using a random number generator to pick the winners ahead of time, and then confirmed the eligibility of the ultimate winner. Participants must register to enter by phone or via the Vax-a-Million website. Teens can register themselves, but parents or legal guardians must verify their eligibility. The names of entrants who don’t win will be carried over week to week. The deadline for new registrations is just before midnight on Sunday. “I know that some may say, ‘DeWine, you’re crazy! This million-dollar drawing idea of yours is a waste of money,’” the governor said when he announced the incentive. But with the vaccine now readily available, the real waste, “is a life lost to COVID-19,” the governor said. The concept seemed to work, at least initially. The number of people in Ohio age 16 and older who received their initial COVID-19 vaccine jumped 33% in the week after the state announced its million-dollar incentive lottery, according to an Associated Press analysis. But the same review also found that vaccination rates are still well below figures from earlier in April and March. More than 5.2 million people in Ohio had at least started the vaccination process as of Monday, or about 45% of the state. About 4.6 million people are done getting vaccinated, or 39% of the state. Nationally, more than 165 million Americans have started the vaccination process, or about nearly 50% of the population. More than 131 million are fully vaccinated, or nearly 40%. Vax-a-Million is open to permanent Ohio residents who have received either the one-dose Johnson & Johnson vaccine or their first part of the two-dose Pfizer or Moderna vaccination. DeWine’s proposal inspired similar vaccine-incentive lotteries in Colorado, Maryland, New York state and Oregon. In Colorado, Democratic Gov. Jared Polis says the state will have a weekly lottery for five residents to win $1 million Tuesday to incentive COVID-19 vaccinations. Colorado is setting aside $5 million of federal coronavirus relief funds that would have gone toward vaccine advertising for five residents to win $1 million each. from https://ift.tt/3oZwz21 Check out https://takiaisfobia.blogspot.com/ The day Dr. Elizabeth Dawson was diagnosed with COVID-19, she awoke feeling as if she had a bad hangover. Four months later, in February 2021, she tested negative for the virus, but her symptoms have only worsened. Dawson is among what “waves and waves” of “long-haul” COVID patients who remain sick long after testing negative for the virus. A significant percentage are suffering from syndromes that few doctors understand or treat. the ranks of patients were swelled by pandemic newcomers. For some, the consequences are life altering. Before last fall, Dawson, 44, a dermatologist from Portland, Oregon, routinely saw 25 to 30 patients a day, cared for her 3-year-old daughter and ran long distances. Today, her heart races when she tries to stand. She has severe headaches, constant nausea, and brain fog so extreme that, she says, it “feels like I have dementia.” Her fatigue is severe: “It’s as if all the energy has been sucked from my soul and my bones.” She can’t stand for more than 10 minutes without feeling dizzy. Through her own research, Dawson recognized she had typical symptoms of postural orthostatic tachycardia syndrome, or POTS, a disorder of the autonomic nervous system, which controls involuntary functions such as heart rate, blood pressure and vein contractions that assist blood flow. It’s a serious condition that sometimes overlaps with autoimmune problems, which involve the immune system attacking healthy cells. Before COVID-19, an estimated 3 million Americans had POTS. Many of those patients report it took them years to find a diagnosis. With her own suspected diagnosis in hand, Dawson soon discovered there were no specialists in autonomic disorders in Portland—in fact, there are only 75 board-certified autonomic disorder doctors in the U.S. The nonprofit organization Dysautonomia International provides a list of a handful of clinics and about 150 U.S. doctors who have been recommended by patients and agreed to be on the list. For people without such connections and knowledge of the medical industry, particularly the low-income people and Black women long-COVID disproportionately affects, appointments typically must be made months in advance. Dr. Peter S. Rowe of Johns Hopkins University in Baltimore, a prominent researcher who has treated POTS and CFS patients for 25 years, says every doctor with expertise in POTS is seeing long-haul COVID patients with POTS, and every long-COVID patient he has seen with CFS also had POTS. He expects the lack of available treatment for these conditions to create a worsening public health scenario. “Decades of neglect of POTS and CFS have set us up to fail miserably,” says Rowe, who also recently authored a paper on how COVID-19 can trigger CFS. A “significant infusion of health care resources and a significant additional research investment” will be needed to address the growing caseload, the American Autonomic Society said in a recent statement. Lauren Stiles, who founded Dysautonomia International in 2012 after being diagnosed with POTS, says patients who have suffered for decades worry about the growing number of people “who need testing and treating but the lack of growth in doctors skilled in autonomic nervous system disorders.” On the other hand, she hopes increasing awareness among physicians will at least get patients with dysautonomia diagnosed more quickly than in the past. Congress has allocated $1.5 billion to the National Institutes of Health over the next four years to study post-COVID-19 conditions, and requests for proposals have already been issued. The National Institutes of Health’s Goldstein says that the miserable experience of the pandemic opens up a unique opportunity for advances in treatment: researchers can study a large sample of people who got the same virus at roughly the same time, yet some recovered and some did not. Long-term symptoms are common among those who were infected with SARS-CoV-2. A published in February in the Journal of the American Medical Association’s Network Open found that 27% of COVID-19 survivors ages 18-39 had persistent symptoms three to nine months after testing negative for the viral disease. The percentage was slightly higher for middle-aged patients, and 43% for patients 65 and over. The most common complaint: persistent fatigue. A Mayo Clinic study published this month found that 80% of long-haulers complained of fatigue and nearly half of “brain fog.” Less common symptoms are inflamed heart muscles, lung function abnormalities and acute kidney problems. Larger studies still need to be conducted to determine the true scale of the issue. However, “even if only a tiny percentage of the millions who contracted COVID suffer long-term consequences,” says Rowe, “we’re talking a huge influx of patients, and we don’t have the clinical capacity to take care of them.” Yet even with these new cases, some physicians discount conditions like POTS and CFS, both much more common in women than men. With no biomarkers, some have argued that the syndromes are sometimes psychological. The experience of POTS patient—and current patient advisory board member of Dysautonomia International—Jaclyn Cinnamon is typical. She became ill in college 13 years ago, and saw dozens of doctors seeking an explanation for her racing heart, severe fatigue, frequent vomiting, fever and other symptoms. For years, without results, she saw specialists in infectious disease, cardiology, allergies, rheumatoid arthritis, endocrinology and alternative medicine—and a psychiatrist, “because some doctors clearly thought I was simply a hysterical woman,” she says. It took three years for her to be diagnosed with POTS. The test is simple: Patients lie down for five minutes and have their blood pressure and heart rate taken. They then either stand or are tilted to 70-80 degrees and their vital signs are retaken. The heart rate of those with POTS will increase by at least 30 beats per minute, and often as much as 120 beats per minute within 10 minutes. POTS and CFS symptoms range from mild to debilitating. The doctor who diagnosed Cinnamon told her he didn’t have the expertise to treat POTS. Nine years after the onset of the illness, she finally received treatment that alleviated her symptoms. Although there are no federally approved drugs for POTS or CFS, experienced physicians use a variety of medicines including fludrocortisone, commonly prescribed for Addison’s disease, that can improve symptoms. Some patients are also helped by specialized physical therapy that first involves a therapist assisting with exercises while the patient is lying down, then later the use of machines that don’t require standing, such as rowing machines and recumbent exercise bicycles. Some recover over time; some do not. Dawson says she can’t imagine the “darkness” experienced by patients who lack her access to a network of health care professionals. A retired endocrinologist urged her to have her adrenal function checked. Dawson discovered that her glands were barely producing cortisol, a hormone critical to vital body functions. Medical progress, she says, is everyone’s best hope. Stiles, whose organization funds research and provides physician and patient resources, is optimistic. “Never in history has every major medical center in the world been studying the same disease at the same time with such urgency and collaboration,” she says. “I’m hoping we’ll understand COVID and post-COVID syndrome in record time.” KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. from https://ift.tt/2SxnZeS Check out https://takiaisfobia.blogspot.com/ As demand for vaccinations drops in the U.S., states are turning to increasingly dramatic measures--Dinner with the governor! Multi-million-dollar lotteries!—to convince people to get their shots. But perhaps the boldest incentive yet has come from the U.S. Centers for Disease Control and Prevention (CDC), which said on May 13 that fully vaccinated people can go maskless, inside and out. The CDC is essentially dangling a carrot: if you get your shot, you can have your regular life back. Lots of experts have questioned whether that strategy will work, and some argue it will backfire. After all, the policy is almost impossible to enforce. There’s little to stop unvaccinated people from going mask-free right alongside those who have had their shots, which could allow the virus to keep spreading. That’s a particular risk in indoor environments, like stores and offices. But a new TIME/Harris Poll survey, conducted May 18-19 among 1,075 U.S. adults ages 18 and older, offers a slightly more optimistic view of the CDC’s gamble. The agency’s policy, Harris found, is motivating some Americans who are getting vaccinated—but not necessarily for the reason you’d think. Among respondents who were either vaccinated in the seven days ahead of Harris’ research or who said they planned to get vaccinated in the near future, 23% said that the CDC’s new mask policy encouraged them to get a shot. That’s a positive, if not massive, effect. But the data also reveal an arguably more interesting finding: among the same group, 41% said they got or plan to get vaccinated at least in part because they’re worried about being around maskless unvaccinated people. The CDC’s new policy probably isn’t the only driver of that feeling—more people are going maskless as case counts drop and states reopen regardless—but it likely played a role. Whether that was the agency’s intended result or not, it does seem that its mask policy is affecting people’s vaccination decisions. from https://ift.tt/34keKkW Check out https://takiaisfobia.blogspot.com/ The Indian government is demanding that social media companies remove all references to the “Indian variant” of COVID-19—saying the term is not scientifically accurate and hurts the country’s image. Tech companies are unlikely to comply with the sweeping request, which would involve removing countless pieces of content including news articles. But it is bringing attention to the problem of how to refer to the COVID-19 variants that are driving many of the new outbreaks across the world without stoking racist or xenophobic sentiments. The demand also comes as Prime Minister Narendra Modi’s government is embarking on a campaign to bring social media sites to heel—even as it grapples with the devastating impact a COVID-19 surge across India. Naming a virusThe World Health Organization (WHO)’s 2015 guidelines warn against naming pathogens after the places where they originate because of a risk of stigmatizing the communities involved. Attacks on people of East Asian origin in the U.S. are rising—which many groups say is the result of former President Donald Trump and others insisting on calling COVID-19 the “China virus.” There are signs that news of India’s outbreak could be similarly sparking hate. Authorities in Singapore denounced an uptick in anti-Indian racism tied to India’s COVID-19 spike after a woman of Indian descent was assaulted there earlier this month. India’s Ministry of Electronics and Information Technology claimed in a May 21 letter that the term “Indian variant” is a misnomer. “It has come to our knowledge that a false statement is being circulated online which implies that an ‘Indian variant’ of coronavirus is spreading across the countries. This is completely FALSE. There is no such variant of COVID-19 scientifically cited as such by the World Health Organization (WHO).” Read more: Why the COVID-19 Variants Spreading in India Are a Global Concern The WHO has advised against using location-based terms for variants, and has designated an official name for the variant first detected in India: B.1.617. The name follows a format indicating the evolutionary relationships between SARS-CoV-2 lineages, similar to the official terms for other variants of concern, such as those first detected in the U.K. (B.1.1.7) and South Africa (B.1.351). But the official designations don’t tend to stick in people’s memories, roll off the tongue easily or make for good headlines. Place names have become widely used as shorthand references for these variants, despite warnings that they are problematic. The WHO says it is working on a new system “that gives variants of concern an easily-recallable name.” But community groups are criticizing the WHO for not moving faster. The organization took six weeks to announce the name “COVID-19” after cases of the coronavirus infection were first reported in Wuhan, China. “I don’t see why it should take so long for them to give this variant a proper name,” says Sabrina Malhi, a spokesperson for the South Asian Journalists Association (SAJA). On May 7, SAJA issued a note to journalists advising publications not to refer to the “Indian variant,” pointing to WHO guidance on the topic. “The former president of the U.S. called coronavirus the ‘China virus’ and we’ve seen an uptick in violence against Asian-Americans, some people say due to that,” she tells TIME. “We didn’t want that happening with the COVID variant that originated in India.” The WHO’s new naming convention will likely be similar to the system used for hurricanes in the U.S., the WHO’s chief scientist Soumya Swaminathan told The Hindu newspaper earlier this month. “It will … be easier for the lay public to remember rather than these complicated lineage numbers,” she said. India clamping down on social mediaSocial media companies were already preparing for a raft of regulations on their platforms to come into effect in India on Wednesday. The rules mandate greater transparency and give users stronger rights to appeal content takedowns. They also stipulate that social media firms must remove content the government says is illegal within three days of being notified, including content that threatens “the interests of the sovereignty and integrity of India,” public order, decency, morality, or incitement to an offense. The companies must also appoint staff members who Indian police can arrest and hold legally accountable if the rules are not followed. But even India’s new Internet rules do not give the government the legal basis to demand such a broad takedown like the removal of “Indian variant.” “But there’s a vague sense of threat which hangs in the air,” says Apar Gupta, executive director of the Internet Freedom Foundation, a New Delhi-based digital rights group. “The rules that are just about to come into force are so onerous and so vague that they give immense power to governments,” he says. “And you obviously don’t want to do something that harms your business interests. So there is a perception of risk, even though there is no legal penalty or requirement to comply with it.” State pressure on social media companies has become increasingly common in India. Last month, amid a devastating wave of COVID-19, the government forced Facebook and Twitter to remove posts by elected lawmakers that were critical of the government’s response to the virus. And on Monday, Indian police stormed Twitter’s New Delhi office after the platform affixed “manipulated media” labels to several posts by members of the ruling Bharatiya Janata Party (BJP). The offices were empty due to pandemic safety measures, but the message to social media platforms operating in India was clear, and broadcast for all to see on national television. from https://ift.tt/2SnJ6QN Check out https://takiaisfobia.blogspot.com/ The vaccines are here. Why do we still need testing? Testing is our eye on the virus. Without testing, we can’t see where it is or where it is going. As fall and winter set in, outbreaks will again occur, sparked by the unvaccinated. And most people become infectious before they know they are infected. Frequent and accessible rapid testing is a tool that if deployed last summer and fall would have saved 100,000 lives. The U.S. missed the opportunity to use frequent rapid testing to stop individuals from unintentionally spreading the lethal SARS-CoV-2 virus to our most vulnerable and avert the horrific winter surge. By rapid tests, I mean the tests that an individual can conduct without a laboratory (ideally in the privacy of their own home) with results given in real-time. There are two types: rapid antigen tests, which look for the virus’s proteins and detect infectious levels of virus. The other lets you know you’ve been infected: rapid molecular tests accurately detect the virus’s RNA and amplify it to confirm infection—sometimes days before the individual shows any symptoms. Despite bipartisan, national support and a call to action from more than 50 leading scientists, the U.S. government has failed to adopt a robust at-home rapid testing strategy that could make these types of tests available to all Americans at little to no cost (similar to what the United Kingdom has done). But the vaccines are here, why do we still need testing? With growing cases around the world particularly due to more transmissible variants, we should be utilizing testing to prevent and control cases and outbreaks when they arise. The new guidance by the CDC, allowing vaccinated individuals to stop social distancing and remove their masks in a wide variety of settings, should have been introduced with complementary at-home rapid testing for all. We’ve seen examples of unvaccinated individuals transmitting to vaccinated residents in nursing homes. We also know that according to the CDC, although a majority of all adult Americans have received at least one dose of the vaccine, the rate of uptake isn’t consistent across the country. In Mississippi, for example, only 31% of the population has received at least one dose. We should be doing everything we can to expand access to the vaccine and convince more people to get vaccinated, but we should also be smarter about testing. We have already seen new variants that spread more quickly and there’s the potential for others to develop increased ability to evade vaccine—derived immunity that could threaten the gains that vaccines have made. When this happens, the virus could find its way into senior centers and nursing homes. Compared to younger individuals, seniors and elderly have somewhat more limited capacity to retain over time highly effective immune protection. By late fall and winter, after almost a year since vaccination, many elderly might again have partially renewed susceptibility. As we navigate the next chapter of the pandemic and work our way closer to normalcy, it is essential that we leverage accurate and highly accessible rapid testing to keep schools, workplaces and travel open in the safest way possible. We know with certainty that individuals don’t need to have symptoms to infect others with COVID-19. The virus presents itself differently in everyone and most individuals are infectious for a number of days before showing any symptoms (if ever). After infection, the virus gets itself situated, before beginning to grow very rapidly. Once it hits its stride, in a single day the virus grows from hundreds of virus particles in the nose, to billions. At that point, transmission can hit its peak, before the person has any recognition that they might be spewing out millions of virus particles with every breath. Symptoms are most frequently a result of the immune response to the virus, rather than from the virus infection itself, and the immune system doesn’t get into full stride and yield fevers until after this peak in virus transmission is achieved. This is a major reason why SARS-CoV-2 has been so difficult to contain—because maximum transmission is often occurring before the body’s sensors kick in to let people know they may be infected. Regular rapid testing can allow contagious individuals to know they are infected and isolate quickly to keep from spreading to others. The White House has focused on vaccines over testing, but why not give each household a box of 20 free rapid at-home tests after a family member gets vaccinated? Surveys show that Americans want accessible, inexpensive (or free) rapid testing. Dr. Fauci has offered his strong support for a robust level of rapid testing many times. In a recent U.S. House Energy and Commerce Hearing, he said, “We should be literally flooding the system with easily accessible, cheap, not needing a prescription, point of care, highly sensitive and highly specific (tests).” At another point, he commented that we as a country have done things “infinitely more complicated” than scaling up rapid tests and getting them into to every household. There are a handful of FDA authorized at-home rapid antigen and molecular tests available for over-the-counter use, but the price point is high and the supply isn’t anywhere near what it should be if we want the majority of Americans to have these tests in their homes. Exactly like we’ve done with the vaccine, the U.S. government should be subsidizing test manufacturing and assisting in the distribution. We know that the combination of vaccines and rapid tests will drive down community transmission to a point where we can effectively eliminate the virus. The time to “flood the system” with rapid tests was 12 months ago. But now is still better than never. We should be investing today in widespread rapid testing to fully reopen the economy, schools and travel safely. Without doing so may well cause more hospitalization and death, and continue to prolong the pandemic. (Mina is a medical advisor to Detect.) from https://ift.tt/3i5MoTN Check out https://takiaisfobia.blogspot.com/ In a release on May 25, Moderna says its vaccine is safe and efficacious among 12- to 18-year olds. The company reported results from its combined Phase 2 and 3 study involving more than 3,700 teens who were randomly assigned to receive either two doses of its COVID-19 vaccine or two doses of placebo. The study was designed to compare results among the teens to those among adults, which led to the company’s current emergency use authorization for its vaccine. Researchers are looking to see if the results among teens are at least as good, and not worse, than those among adults. And that’s what the company reported. There were no cases of COVID-19 reported 14 days after the teenage study participants received two doses of the shot, compared to four cases among those receiving a placebo, meaning the vaccine was 100% efficacious in protecting against disease. The company said that the vaccine was also 93% efficacious in protecting against even one symptom of COVID-19 disease after one dose. Moderna is the second company to report COVID-19 vaccine results among teens; in March, Pfizer-BioNTech reported similar safety and efficacy of 100% in its study and received authorization from the FDA for its two-dose shot among teens in May. Both Moderna and Pfizer-BioNTech vaccines are built on mRNA technology, which involves using genetic material from the COVID-19 virus to train the immune system to fight it. Moderna plans to submit the latest data from the teens to the U.S. Food and Drug Administration to expand the current authorization for its vaccine to children as young as 12 years old.
from https://ift.tt/34h0Pfy Check out https://takiaisfobia.blogspot.com/ The darkness descends slowly for people with retinitis pigmentosa (RP), a degenerative eye disease that affects 2 million people worldwide. The condition is typically diagnosed in childhood or adolescence, but it can take until middle age before a person’s vision has deteriorated severely enough that they are fully or effectively blind. When the lights finally do go out, however, they stay out. Or that’s the way things used to be. In a breakthrough study published today in Nature Medicine, investigators report a relatively simple yet remarkably effective way to restore partial vision to RP patients—one that, with further study, may soon have wide application. The key lies in the rod-shaped photoreceptors that principally govern peripheral vision and the cone-shaped receptors that give us our central view of the world. In people with RP, mutations in more than 70 genes cause slow deterioration of the rods, leading to tunnel vision, and later the cones, leading to blindness. Light still streams into the eye through the unaffected lens, and that light could still make its way to the brain via the optic nerve. But the retina, which lies between the two, no longer works. A team of researchers, led by Dr. José-Alain Sahel, professor of ophthalmology at Sorbonne University and the University of Pittsburgh, however, thought they might have a way to bring the retina back into the game: ChrimsonR, a protein that opens electrical channels in neurons and makes them reactive to light. The trick was finding a way to deliver the protein—and the answer was to genetically manipulate a harmless adenovirus so that it carried ChrimsonR; the virus was then injected into the fluid-filled portion of the eye behind the lens. “The ChrimsonR sparks electrical activity,” says Sahel. “It transforms the cells and makes them able to absorb light, though it takes a while—about four months—for the cells to take up the virus and the protein with it.” Nonhuman primate studies showed that the technique did not harm the eye, and also helped the researchers establish the proper dose of Chrimson4 to sensitize the retinal cells. For the human trial, Sahel and his team worked with a 58-year-old man who had been diagnosed with RP 40 years earlier and whose vision was limited to rudimentary light perception. They treated the poorer functioning of his two eyes—in order to spare the marginally healthier one if anything went wrong with the experiment—and injected it with a single dose of the altered virus. Assuming the experiment worked, the next steps would not be nearly so simple as waiting the required four months or so until the man’s vision simply returned in the treated eye. ChrimsonR is not remotely sufficient to restore the exquisitely complex interplay of rods and cones that give healthy eyes their rich, colorful, three-dimensional view of the world. Rather, it sensitizes cells mostly in the amber spectrum, making shapes and shadows discernible at that color frequency. What’s more, a healthy retina reacts in real time to the amount and intensity of light striking it, becoming more reactive in low-light conditions and less reactive in bright light, to prevent damage to retinal cells. To see at all through the treated eye, the patient needs to wear a pair of goggles that shifts incoming light to the amber spectrum and regulates it to a safe intensity. “The eye needs a lot of light, but there is the danger that it could be a toxic level,” says Sahel. “Without the goggles it could be like the patient looking directly into the sun.” While waiting for the ChrimsonR to take effect, members of Sahel’s team worked with the patient, training him with the goggles and running tests to see if he could distinguish objects placed on a table, point to them, count them, and pick them up. Over repeated trials, there were no results—until finally, as Sahel recalls it, he got a call from one of his team members with a simple message: “He sees.” At right around the four-month mark, the subject began achieving remarkable results on all of the lab tests. And in the months since that breakthrough, he has become able to navigate his world in new ways: he can detect the crosswalk at an intersection and count the number of white stripes demarcating it; perceive objects like a plate, a mug and a phone; spot a piece of furniture in a room and see a door in a corridor. “He can also,” adds Sahel, “detect where people are.” Sahel believes the results will be long-lasting, or even close to permanent. “We think this could last at least 10 years or it could be for a lifetime,” he says. “If not, we can always go back and re-inject.” As to whether the treatment is ready for practical application beyond the one patient, Sahel says the answer is “a small yes and a big no.” The small yes is that the work was merely a feasibility study (but by any measure, it succeeded spectacularly). The big no is that a great deal more research must be conducted to learn more about dosing levels, to improve both the goggles and the training patients go through to use them, and to figure out when in the course of a person’s RP is the right time to begin the treatment—Sahel notes that for now, at least the procedure is only for people with very advanced disease. “People with RP can retain central vision for many years,” he says. “You always have to weigh the benefit versus the risk.” from https://ift.tt/3yv3kZD Check out https://takiaisfobia.blogspot.com/ The U.S. Centers for Disease Control and Prevention’s (CDC) announcement last week that fully vaccinated people no longer have to wear masks or socially distance came as a great relief to millions of people who have been vaccinated. But it has also led to confusion and chaos in workplaces and other locations where vaccinated and unvaccinated people mix. Public health agencies like CDC are charged with protecting the health of populations, not just individuals. With its recent masking recommendation, the CDC is forgetting its basic public health mission, holding back our efforts to stop the COVID-19 pandemic, and increasing the danger that workers face. Workplaces are centers of virus transmission, and those who work in such environments have borne a tragic burden throughout the pandemic. While most white-collar workers have sheltered at home, performing their job tasks on Zoom and other video platforms, workers in health care, transportation, food processing, corrections, retail and other essential jobs have been forced to come to work every day, risking their safety and the safety of their loved ones. While we may never know the exact number of work-related infections or deaths from COVID-19, we do know that the pandemic has taken a devastating toll on workers across key sectors. Major outbreaks across the country have been traced to virus transmission in meat processing, grocery stores, warehouses, farms and factories, where workers are in close proximity to each other or members of the public. One of the groups hit hardest by the pandemic are workers at long-term care facilities. according to data from the Centers for Medicare & Medicaid Services (CMS). Not all “essential” workers are equally at risk. Black and Brown workers are overrepresented in workplaces with the highest risk or exposure. This is one of the primary reasons working-age adults from minority communities in the U.S. are so much more likely to be sickened or killed by the virus than white Americans of the same age. Since the earliest days of the pandemic, worker advocates and public health experts have been asking the Occupational Safety and Health Administration (OSHA) to issue mandatory, enforceable emergency standards to supplement CDC’s voluntary guidance. The Trump Administration refused to allow OSHA to do so. But just two days after being sworn in as President, Joe Biden issued an executive order calling for OSHA to issue such a standard by March 15. Now, more than two months after President Biden’s deadline, OSHA still has not issued this badly needed regulation and the CDC’s recent announcement is making an already bad situation worse for workers. The CDC said its new guidelines do not apply to health care, corrections, homeless shelters and transportation, but there are many other types of workplaces with similarly dangerous working conditions—like where large numbers of workers have been infected in the recent past and in which outbreaks continue to occur. In failing to consult with workplace experts before issuing its guidance, the CDC has managed to infuriate both labor unions and employers. The United Food and Commercial Workers union, which represents meat processing and grocery workers,The Retail Industry Leaders Association, a trade group, States and localities can maintain public health precautions, but after the CDC’s announcement, most governors have abandoned them. Many have already done so, despite the fact that . In states where that’s happened, it is now on the honor system whether a worker or customer discloses whether or not they’ve been vaccinated—and how well a worker is protected is essentially up to their employer. Workers employed by Albertsons or Whole Foods, which are maintaining their mask requirements, will be better protected than workers at Walmart or Trader Joe’s, which have lifted theirs. Employers who want to do the right thing feel handcuffed, their options limited by existing Equal Employment Opportunities Commission (EEOC) regulations that prohibit them from requiring every employee to be vaccinated—employees can refuse if they have a disability or religious-related objection. Lower-wage, as well as Black and Brown workers are less likely to have been vaccinated than higher-wage and White workers—and for many, the reason is not “vaccine hesitancy,” but structural barriers to getting the shot, like a dearth of transportation options, difficulty in missing work to get a vaccine, health issues, language barriers, fear of having to pay out of pocket for the vaccine and concerns stemming from legal status, particularly for Hispanic workers. CDC needs to work with OSHA, EEOC, unions, and employer organizations who understand workplaces better than CDC scientists to establish criteria for when it is safe to relax protections in high-risk workplaces—especially in areas where community transmission remains high. OSHA should then be given authority to require workplace outbreak reporting and, when exposure risk is high, and require employers to apply The CDC has exempted certain high-risk workplaces from its new guidance, telling operators of healthcare facilities, correctional or detention facilities and homeless shelters to continue to provide masking and other precautionary measures for all vaccinated and unvaccinated people: employees and members of the public. The types of workplaces where precautionary measures remain Unlike the general public who may spend 20 minutes in a grocery store or on a bus, or an hour in a restaurant, many workers spend 8-12 hours a day at work with frequent or prolonged close contact with each other or the public in poorly ventilated indoor settings or enclosed spaces, like meat processing plants where employees work elbow to elbow; retail stores where workers have hours of contact with the public; and factories and warehouses where large numbers of workers congregate indoors. Finally, benchmarks need to be established for when it is safe and appropriate to step down mitigation measures as infections decline and vaccinations increase in communities. Measures would remain in workplaces with active outbreaks of COVID-19, in locations where community transmission of COVID-19 is high, or workplaces where not all workers are fully vaccinated. The CDC made a mistake. Public health agencies need to follow the science for protecting populations, not just individuals. But it is not too late to fix that mistake and get the nation’s pandemic control efforts back on track. from https://ift.tt/3wu2QB9 Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 Well hello! I’m so glad you’re here. A version of this article also appeared in the
Well hello! I’m so glad you’re here. A version of this article also appeared in the RSS Feed
RSS Feed
