|
If the Supreme Court overturns Roe v. Wade this summer, as a leaked draft opinion suggests it may, abortion will likely be banned or severely restricted in about half of the United States. But that doesn’t necessarily mean the country will return to a world before 1973, when the landmark Supreme Court case enshrined a constitutional right to abortion. Abortion pills, which can be ordered online and delivered by mail, have already fundamentally changed reproductive rights in America. The regimen of two drugs, mifepristone and misoprostol, can in theory be safely taken anywhere, including in the privacy of people’s homes, eliminating the need to undergo a procedure, travel out of state, take time off work, or confront protestors outside of a clinic. In part because of this convenience, abortion pills—also known as medication abortion—are now the most common method of ending a pregnancy in the U.S. But abortion rights advocates say that huge obstacles remain in accessing these drugs. Due to a complicated patchwork of legal and regulatory hurdles in different states, combined with societal issues such as poverty and a lack of internet access, many would-be patients either have never heard of abortion pills, or don’t know where to get them, how to take them safely, and whether they’re legal. Medical professionals are often similarly flummoxed. Many who do not currently provide abortions know little about the pills themselves, and abortion providers, who are operating with very few resources, must navigate a maze of misinformation and ever-shifting legal risks on behalf of themselves and their patients. Conservative lawmakers in 19 states have further complicated legal questions by passing laws that effectively prohibit the use of telemedicine and limit where the pills can be administered. Amid this confusing landscape, many are turning to the internet, where they’re confronted with different problems: misleading information, websites designed to mimic reliable organizations, and platforms that can collect their data and take more knowledge to safely navigate. With the Supreme Court poised to overturn Roe and Republican-led states passing ever-more restrictive laws, abortion rights advocates are racing to get ahead of the curve. In the last few months, advocacy groups have published online guides to obtaining abortion pills, purchased ad campaigns on the New York City subway, and launched online courses on how to “self-manage” abortions outside the established health care system. Internet privacy experts have posted toolkits to help individuals protect their digital footprints, and staffed up hotlines that answer medical questions from people taking abortion pills in anticipation of an increase in need. Groups that fund abortions are also raising millions of dollars to help subsidize or cover the cost of the pills for individuals, and to help people travel to states where it will stay legal for providers to prescribe them. Physician organizations are funding programs for medical residents to learn about medication abortion, and encouraging a broad array of doctors to get up to speed on abortion pills, the legal atmosphere around them, and the misinformation that is already starting to circulate online and in state houses around the country. Elisa Wells, co-founder of Plan C, an organization dedicated to spreading information about how to access and take abortion pills, says medication abortion will be crucial in any post-Roe era. “One of the huge differences between then and now is that you do have these pills, they are in our communities, they are accessible through the internet,” she says. “And we hope that will at least lead to medically safe access to care even when it is restricted.” A push to inform patients and medical staff about abortion pillsThe number of medication abortions has been steadily increasing since mifepristone was approved by the U.S. Food and Drug Administration (FDA) in 2000. In the U.S., the vast majority of abortions are completed at or before 13 weeks of pregnancy—so abortion pills, which are approved for use up to 10 weeks, are an option for many patients. In 2020, the pills accounted for 54% of U.S. abortions. The uptick was due in part to the COVID-19 pandemic, during which time conservative states forced some brick-and-mortar clinics to temporarily close and access to telehealth appointments increased. Another major factor was an FDA decision in April 2021 to lift restrictions on mailing abortion pills during the pandemic; in December, it extended that policy permanently. 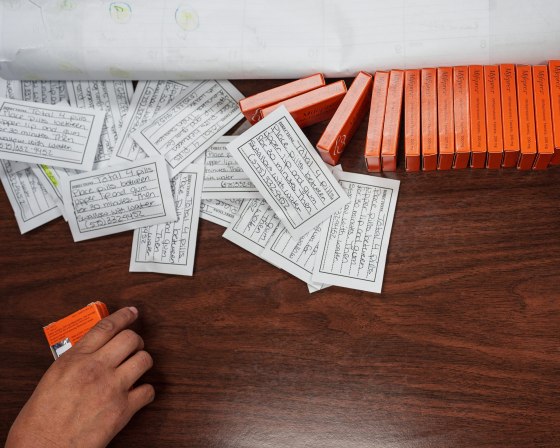
But if the use of medication abortion has increased, access to the drugs has been unevenly distributed, says Ushma Upadhyay, an associate professor at the University of California, San Francisco, who is leading a study of the use of telehealth for abortion pills in 22 states. “There are many people who don’t know that abortion pills even exist,” she says. “If they do know that abortion pills exist, they don’t know that they can access them through telehealth without an in-person visit, that they don’t have to tell many people about their decision.” Only about 1 in 5 adults had heard of medication abortion in 2020, according to the nonpartisan Kaiser Family Foundation (KFF). People of color, immigrants, those who live in rural areas, and teenagers are disproportionately unlikely to have access to abortion pills, says Upadhyay. None of the three major medication abortion telehealth companies in her study take Medicaid or offer services in languages other than English, and other companies have similar barriers. Black and Hispanic Americans, low-income people, and those who live far away from cities are less likely to have broadband internet at home, and therefore may struggle to get a prescription via telehealth. Nearly two-thirds of the first 3,200 patients who have received abortion pills in Upadhyay’s study are white, compared to the national population of abortion patients, which is about 40% white. Upadhyay’s research also shows that 82% of those who have accessed abortion pills live in urban areas and nearly 75% were between 18 and 34 years old. The challenges of accessing abortion pills in states that ban abortionWhile medication abortion is not yet illegal in any state other than Oklahoma which just passed a law banning all abortion from the moment of “fertilization,” legislators in 22 states have introduced a flurry of new bills since January that would severely restrict access to or outright ban abortion pills. Many states have already passed laws requiring the prescribing clinician to be physically present when the pills are administered, effectively banning telehealth appointments in which abortion pills are prescribed, then mailed to a patient. Some have also explicitly banned telehealth for abortions. Three states outlaw self-managed abortion. And while lawmakers have otherwise traditionally targeted abortion providers rather than patients, abortion pills--which patients can get by mail or can order online without a doctor’s involvement—complicate that dynamic. Not only is it more difficult for officials to enforce laws against providers who don’t live in their state, but the impending Supreme Court decision has also emboldened some anti-abortion lawmakers. On May 4, two days after the Supreme Court leak, lawmakers in Louisiana advanced legislation that would classify all abortion—including medication abortion—as homicide and allow prosecutors to charge patients. While that bill is extreme by any measure, even states that don’t explicitly criminalize patient actions could expose individuals to legal risk. The arrest of 26-year-old Lizelle Herrera in Texas last month over an alleged self-managed abortion raised concerns about how officials will treat people in states with abortion restrictions on the books. Staff at the hospital where Herrera sought care reported her to law enforcement, resulting in a temporary murder charge. While authorities ultimately dropped the charge, she spent three days in jail. Texas has banned abortions after about six weeks of pregnancy, but that law carries no criminal punishment for individuals who seek out abortions, and no other law applied in this case either. “I worry about the chilling effect,” says Cynthia Conti-Cook, a civil rights attorney and technology fellow at the Ford Foundation. “The people who are most likely to be targeted for investigation, surveilled and prosecuted … are communities that are majority Black people and immigrant communities, and communities that in any other way have experienced historical oppression.” Leah Coplon, a certified nurse midwife and director of clinical operations at Abortion on Demand, a group that provides abortion pills by mail in 21 states, says patients ask her about legal liability. While Abortion on Demand only mails pills in states where it is legal to do so, some patients are concerned about scrutiny from health care or law enforcement officials, while others worry their own friends and family, who might not support their decision to get an abortion, could take action to stop them. Coplon explains that because the outcome of a medication abortion looks exactly like a miscarriage, and can be treated as such in a health care setting, patients don’t have to tell anyone they have taken the pills. Patients who live in any of the 19 states where mailing abortion pills is restricted can still access the pills from an in-person clinic or from international services like the Austrian-based Aid Access, a group founded by Dutch physician Dr. Rebecca Gomperts, which ships abortion pills to all 50 states. For patients in states where mailing pills is legal, Gomperts works with nine U.S.-based providers, and for those in restricted states, she prescribes the pills herself and sources them from a pharmacy in India. In 2019, the FDA demanded that Aid Access stop, saying the generic mifepristone was a “misbranded and unapproved drug,” but Aid Access sued the agency and the FDA ultimately did not take further action against the organization. 
Some U.S. providers are also finding workarounds. Dr. Julie Amaon, medical director of telehealth abortion pill company Just the Pill, sometimes tells patients to drive to the nearest state that allows pills to be prescribed by telehealth. She then arranges for the pills to be sent to FedEx, UPS, or Post Office pickup points. Just the Pill is also planning to staff mobile clinics that will travel to states, including Illinois, Pennsylvania, and New Mexico, where abortion will likely remain legal but that border states with strict anti-abortion laws. Such mobile clinics will help “offload all the medication abortions so [brick-and-mortar clinics] can focus on procedures,” Amaon says. Hey Jane, another telehealth medication abortion company, similarly ships to Post Office boxes and other pickup points in states where abortion is likely to remain broadly legal, including New York, California, Washington, Illinois, Colorado, and New Mexico. Hey Jane CEO Kiki Freedman says she chose those states because they are places that expect to see an influx of patients as GOP-led states ban abortion. Educating via social media is both crucial and problematicMelissa Grant, an executive at Carafem, another company that remotely provides abortion pills, says stigma and misinformation can be almost as problematic as legal restrictions. “You might say, ‘I have a great dentist,’ but it’s rare you’d say, ‘Hey, this is a great place to have an abortion,’” Grant says. “We’ve had to find ways to reach people and let them know we’re not a crisis pregnancy center, we’re real, and you can come here and trust us.” To that end, Carafem operates a text-message support service to answer patient questions as they self-manage abortions. Other hotlines, including the Repro Legal Helpline and the Miscarriage and Abortion Hotline, which recently increased its team from 40 to 50 volunteers, provide similar support. Other abortion rights advocates are working to seed search and social media platforms with reliable information. Plan C has built an online directory where people in all 50 states can find services that will send them abortion pills by mail. It also provides information about each state’s laws, as well as the potential legal risks that patients face. Plan C also posts artwork, information, and paid ads about medication abortion across social media platforms. The day after the Supreme Court draft leaked, Plan C saw a huge spike in traffic to its site, reaching 56,000 visitors, up from an average of 2,300 a day before the leak. “The internet is clearly a huge improvement [from the pre-Roe era] in a lot of ways, and a powerful tool in our ability to share information,” says Wells, Plan C’s co-founder and co-director. But such information is only useful to those who are able to find it in the first place. Many would-be abortion patients either don’t have private access to the internet, or are fearful that their online search histories could leave them exposed to legal liability, providers and scholars say. Some groups have posted guides to help people protect their data when searching for information about abortions. Others have taken steps to combat disinformation disseminated by anti-abortion groups, which regularly use phrases and imagery in their online advertisements designed to lure people in search of information about abortion, in order to deter them from ending their pregnancies. Websites for anti-abortion pregnancy centers often feature FAQs about medication abortion, for example, but include warnings that it can be dangerous or encourage people to make an appointment to learn more. Only the fine print clarifies that they do not offer abortions. Other anti-abortion groups also promote “abortion pill reversal” treatments, an idea that the American College of Obstetricians and Gynecologists says is “not based on science.” Plan C and other abortion rights advocates say that social media platforms, including Facebook and Instagram, frequently remove their posts, refuse to run ads, or deprioritize their pages with little or no explanation. For example, just days before a Texas law banning abortion after about six weeks took effect last fall, Plan C’s Instagram account was suspended; Plan C was notified it had violated the platform’s community guidelines or terms of use, Wells says. Many of its advertisements and posts still get taken down by Instagram and Facebook, says Martha Dimitratou, Plan C’s social media manager. Facebook ads with language like “there is a safe alternative to in-clinic abortion” and “abortion pills belong in the hands of people who need them” are rejected for violating a Facebook policy that bans ads promoting the sale or use of “unsafe substances,” according to screenshots provided by Dimitratou. An ad promoting an event last month training people on medication abortion and self-managed abortion was rejected for the same reason. Meta, the parent company of Facebook and Instagram, declined to answer questions about Plan C or other groups’ posts. A spokesperson for Meta said its platforms allow posts and ads that raise awareness of abortion and provide information about abortion, including abortion pills, but the company does not allow direct sales of prescription drugs. All abortion content must also follow the platforms’ policies on topics such as prescription drugs, misinformation, and bullying and harassment. Dimitratou calls the policies “counterproductive.” “You have to spend a lot of time just through the whole process appealing things and trying to convince them that abortion pills are legal and safe,” she says. Aid Access has experienced similar problems, says Christie Pitney, a certified nurse midwife who works with the group to prescribe abortion pills in states where telehealth for abortion is legal and helps run the group’s social media. On May 10, as it was seeing a surge in interest following the Supreme Court leak, Aid Access’s Instagram account was suspended, Pitney says. It has since been restored, but she and Gomperts say other issues are ongoing. Women on Web, another group founded by Gomperts that mails abortion pills all around the world, has seen its Facebook and Instagram ads rejected too, according to screenshots provided by Dimitratou, who runs social media there as well. When Google updated its algorithm in May 2020, Women on Web appeared farther down in search results, leading to a 75% drop in traffic, according to Dimitratou. “How do you make sure that all the people that need you can find you? That’s what is so damaging about these laws. It will make it so difficult for people to find information,” Gomperts says. “When it’s illegal, nobody is there to give that information anymore and it becomes such a taboo. And that is internalized so that people are scared, and they don’t dare to talk about it anymore. And then information becomes much harder to find.” A Google spokesperson told TIME that its algorithm changes are not designed to penalize or benefit any one site. “Our Search ranking systems are designed to return relevant results from the most reliable sources, and on critical topics related to health matters, we place an even greater emphasis on signals of reliability,” the spokesperson said. “We give site owners and content producers ample notice of relevant updates along with actionable guidance.” In other countries where abortion is tightly restricted, including Poland and Saudi Arabia, Google does not allow abortion-related ads, and social media posts in some places are more limited too. It’s unclear how tech companies will handle ads in the U.S. if some states outlaw abortion entirely, as they’re widely expected to do. A coalition of abortion rights groups and providers plans to meet at a digital rights conference in June to share strategies for navigating the complex world of social media policies and develop a list of improvements they would like to see from Big Tech companies. In the meantime, many groups are making an effort to reach people offline. Local abortion rights activists have held trainings on self-managing abortion for months. Last August, Plan C activists drove a truck around Texas with a mobile billboard advertising abortion pills, and this spring, the group paid for colorful ads on the New York City subway. 
A new frontline: family doctors and others who don’t perform abortionsDr. Chelsea Faso, a New York City-based family medicine physician who works with the nonprofit group Physicians for Reproductive Health, says there’s also a need to educate health care providers. Abortion, she says, should be treated no differently than other types of medical care. “Most family docs, like myself, provide care for folks from the cradle until they’re approaching the end of life,” Faso says. “When folks come in with a pregnancy, it really is our responsibility to be able to counsel that person on all of their options.” Several organizations have taken the message to heart. Innovating Education in Reproductive Health, a program at the UCSF Bixby Center for Global and Reproductive Health, has launched a video series to educate providers in states where abortion is severely restricted on how to care for patients who self-manage their abortions. Reproductive Health Education in Family Medicine (RHEDI) tries to spread that message early, by providing funding and support for family medicine residency programs that want to include abortion care in their curricula. Some “medical students are surprised to know that you can be a family medicine doc or a primary care doc and provide abortions,” says Erica Chong, RHEDI’s executive director. “That’s the first hurdle to get over.” In 1997, a few years before the FDA approved mifepristone, about half of U.S. family medicine doctors surveyed by KFF said they were interested in offering the drug to patients. Decades later, only about 3% of early-career family doctors actually provide abortions, according to a 2020 study published in Family Medicine. Among that group, about 40% signaled that they provided only medication abortions, as opposed to procedural abortions. Dr. Emily Godfrey, an abortion provider and family medicine physician at the University of Washington, says regulatory constraints are part of the problem. Even though it has repeatedly been shown to be safe, mifepristone is subject to the FDA’s Risk Evaluation and Mitigation Strategies program, which places safeguards on drugs that regulators think pose potential risks. Under that program, providers have to register before they prescribe mifepristone, and that extra step can be a significant barrier, particularly for those who work in religiously affiliated health systems that do not provide abortion care, Godfrey says. More than 30 states also require a physician’s prescription, shrinking the provider pool to exclude nurse practitioners, physician assistants, and other clinicians. Because mifepristone is closely regulated by the FDA, some providers are wary of offering it, says Ian Lague, the curriculum and program manager at RHEDI. “A lot of it is a confidence issue,” Lague says. “People feel that they need more training”—even when they’re perfectly qualified. Studies show the pills are 95% effective, and with a complication rate of less than 1%, they are safer than Tylenol or Viagra. Legal requirements present another barrier. In Utah, for example, doctors are required to tell patients that medication abortion is reversible. Other laws, including ones in Texas and Oklahoma, also make anyone who aids an abortion liable to legal action, so “there’s a lot of fear to even talk about it or refer patients,” says Cindy Adam, CEO of the medication abortion provider Choix. Some advocacy groups, including local abortion funds, are reminding doctors about their rights, and encouraging medical professionals not to report patients who may have had an abortion to the authorities. Even in states where people who enable an abortion can be legally vulnerable, doctors are not required to report patients to the police if they suspect they’ve taken abortion pills. “We have to, as a medical community, reinforce that fact,” Faso says. “There is no mandated reporting law for this and you are violating” patient privacy if you report someone. Even with all of this knowledge and preparation, advocates and providers say it’s hard to predict exactly what they’ll see if Roe is overturned. Some Democrat-led states are making moves to protect abortion providers and increase funding for the procedure. The manufacturer of generic mifepristone is challenging Mississippi’s abortion pill restrictions in a case with a hearing scheduled June 8. Pitney, the Aid Access provider, says that medication abortion will likely reduce the number of people required to travel out of state to access abortions, but calls it a “Band-Aid on a much larger problem of access.” She predicts that unsafe abortion will increase if Roe is overturned, and that abortion providers, many of whom have been working on shoestring budgets for years, will struggle to offer services. “The abortion community was stretched thin prior to this,” Pitney says. “But the work is gonna get harder.” Aid Access’s Gomperts says that so far U.S. laws have not prevented her from mailing pills to any state. But even if lawmakers double-down and do try to prevent her from serving the U.S., the existence of safe, effective abortion pills means that the genie is out of the bottle. “They might be able to stop me, but that doesn’t mean that they will be able to stop medication abortion,” Gomperts says. “You cannot stop women accessing safe abortions with pills. They’re never going to stop that.” from https://ift.tt/kWls5AZ Check out https://takiaisfobia.blogspot.com/
0 Comments
In mid-May, I traveled from London to Slovenia to interview the Ukrainian men’s soccer team on their bid to reach November’s Qatar World Cup. It was a four-day assignment, requiring travel via train stations, airports, and taxi ranks—but at no point was I asked to show a negative COVID-19 test, my vaccination status, nor even to wear a facemask. I can barely recall seeing anyone wear one, least of all the elite sportsmen with whom I mingled daily. It was equally refreshing and disconcerting—as if Europe had forgotten that the pandemic had ever happened and was indeed still happening. [time-brightcove not-tgx=”true”] It was on this trip that a news alert flashed on my phone: China, on May 14, announced it was withdrawing from hosting the Asian Football Confederation Cup—the continent’s premier international soccer tournament—due to a COVID-19 outbreak that, on that same day, was responsible for only 65,000 cases and 45 deaths nationwide. That China is still wedded to a stringent zero-COVID policy focused on stamping out every infection, rather than mitigating severe illness and deaths, wasn’t a secret to anyone following the harsh lockdown endured by the 26 million residents of Shanghai, its biggest city, over the last two months. Still, it was surprising because Beijing, not too long ago, hosted the 2022 Winter Olympics without seeding a major outbreak and China’s leadership relishes in the prestige that accompanies these major sporting events. But what caught my eye most was the timing: the nixed tournament didn’t kick off until June 2023. What it suggests is that China has no intention of following the West into a vaccine-powered “living with the virus” dynamic. That’s bad news for China’s own economy and for any diminishing hopes worldwide of avoiding a global recession. Over the last two decades, China has contributed a quarter of the rise in global GDP—in that time, the first quarter of 2020 was the only one when its economy did not expand. Today, however, more than 200 million Chinese live under pandemic restrictions, battering an already slowing economy. Retail sales in April were 11% lower year-on-year, while housing sales—comprising over a fifth of GDP—plummeted 47% over the same period. Unemployment across a sample of 31 major Chinese cities is now the highest per official data since records began in 2018. Scenes from early May of workers fighting with public health officials at a factory producing Apple MacBooks in Shanghai after they were refused permission to leave their workplace to rest at on-site dormitories spotlights the mounting friction between economic priorities and public health. “Ordinary Chinese people have felt the heavy-handed authoritarianism of the Party in a much more direct and personal way than many people, especially young people, have before,” says Astrid Nordin, the Lau Chair of Chinese International Relations at Kings College London. Read more: China, Isolated From the World, Is Now the Last Major Country Still Pursuing a ‘Zero COVID’ Strategy Since China began market reforms in the late 1970s, its ruling Chinese Communist Party (CCP) has rooted its legitimacy in improving livelihoods. But over the last two years, President Xi Jinping has seized on China’s success conquering the virus as proof of the superiority of its political system over the West. These two success stories are now in direct conflict. On May 25, Chinese Premier Li Keqiang held an emergency meeting with over 100,000 party members where he warned China’s current economic woes were in some ways greater than the initial impact of the pandemic in 2020 and indicated that the annual growth target of 5.5% was unobtainable. “The economic crisis owing to draconian measures to control the outbreak really shows the mess, miscoordination, and miscalculations by leadership at the top,” says Valerie Tan, an analyst on Chinese elite politics for the Mercator Institute for China Studies in Berlin. “We’re finally seeing the full manifestation of this ideological turn by Xi Jinping.” Still, nobody expects Beijing to abandon its zero-COVID policy anytime soon. It’s especially sensitive for Xi as the 20th CCP Congress approaches in the fall, when the strongman is expected to assume a third five-year presidential term, ripping up the longstanding convention that leaders only serve two. The prospect of COVID-19 running amok while he takes this historic step won’t be countenanced. On May 5, the CCP’s Politburo’s standing committee, China’s apex political body, said zero-COVID was “determined by the nature and purpose of the Party,” thus expressly linking it with CCP legitimacy, while declaring that relaxing controls would lead to “massive numbers of infections, critical cases and deaths.” Despite the ideological nature of China’s zero-COVID obsession, this grim prognosis is not hyperbole. According to a study published May 10 by researchers from Shanghai’s Fudan University, Indiana University, and the U.S. National Institutes of Health, relaxing COVID-19 restrictions in China could lead to 112 million cases and 1.5 million deaths in just three months. This is above all because China has not fully vaccinated 100 million of its 264 million citizens over 60, or 38%. In semi-autonomous Hong Kong, a wave of the highly transmissible Omicron variant led to some of the world’s worst daily mortality rates in recent months, with 95% of those deaths in over-60s who hadn’t been fully vaccinated. Read more: How Hong Kong Became China’s Biggest COVID-19 Problem In this regard, China is a victim both of its success in stemming the spread of less transmissible variants and of its backslapping propaganda. Elderly people with scant desire to travel abroad saw no need to get vaccinated against a virus that the state had triumphantly declared vanquished. Meanwhile, owing to a pernicious blend of national security and national pride, China has not approved any foreign vaccines, meaning it doesn’t have access to the most effective types, which are those based on mRNA technology. Homegrown alternatives have spotty efficacy. Not that it really matters in a place where zero-COVID is the iron-clad law of the land. Even the best COVID-19 vaccines do not eliminate transmission, but they do slow the spread and drastically reduce the severity of symptoms. However, that renders them incompatible with any zero-COVID strategy, which doesn’t differentiate between mild or severe cases, or those in young and old. The policy targets infections, period, not sickness or deaths. “This is why it’s so political,” says Dr. Yanzhong Huang, senior fellow for global health at the New York City–based Council on Foreign Relations. “Unless they abandon their zero-COVID mindset there’s really no way out of this.” Little wonder even the WHO says that zero-COVID is unsustainable. The Chinese public are wising up to this fact and complaints about the government’s handling of the pandemic have become common even on the nation’s heavily censored social media. This has led to a new official edict: jingmo, or silence. Stop grumbling, in other words. During that May 5 Politburo standing committee meeting, Xi vowed to crack down on “all words and deeds that distort, doubt, and deny our epidemic prevention policies.” Ominously, China’s National Health Commission chief Ma Xiaowei wrote in CCP ideological journal Qiushi on May 16 that more “permanent” quarantine hospitals must be built and weekly testing “normalized.” Not hosting the AFC Cup won’t do much damage to China’s global reputation. But rolling lockdowns, which are sending China’s factories screeching to a halt, with cascading detrimental effects all the way down global supply chains, will make commercial partners look elsewhere. In Shanghai, China’s biggest port responsible for one-fifth of the country’s international shipping, average waiting time for import containers was 12.9 days on May 12, up from 7.4 days compared to six weeks earlier, according to shipment tracker Project 44. Over half of American businesses in China either delayed or decreased investments in China due to lockdown measures, according to a recent survey by the local U.S. Chamber of Commerce. Thanks to current measures, “China might be seen as a less reliable trading partner than previously,” says Nordin, of Kings College. “The question is how much less reliable than other possible alternatives?” from https://ift.tt/cx1PDSf Check out https://takiaisfobia.blogspot.com/ U.S. and Canadian regulators are investigating a hepatitis outbreak that may be linked to fresh organic strawberries. In a joint weekend statement, the U.S. Food and Drug Administration and the Public Health Agency of Canada said illnesses in Minnesota, California, and Canada occurred after people consumed FreshKampo and H-E-B brand strawberries. The agencies said the strawberries were purchased between March 5 and April 25. They were sold at various U.S. retailers, including Aldi, Kroger, Safeway, Walmart, and Trader Joe’s. In Canada, the affected strawberries were sold between March 5-9 at Co-op stores in Alberta and Saskatchewan. The potentially affected strawberries are past their shelf life, but health officials say consumers who purchased them and froze them to eat later should throw them away. There have been 17 illnesses and 12 hospitalizations reported in the U.S., the FDA said. Ten cases and four hospitalizations have been reported in Canada. Mexico-based FreshKampo, which grew the strawberries, said in a statement Sunday that it is working with regulators to determine how the problem occurred. FreshKampo said the label on the containers of potentially affected strawberries would have said “Product of Mexico” or “Distributed by Meridien Foods.” In a statement on its website, Texas grocer H-E-B said it has not received or sold organic strawberries from the supplier in question since April 16. H-E-B said anyone who still has the strawberries should throw them away or return them to the store where they were purchased. Hepatitis A is a virus that can cause liver disease and, in rare cases, liver failure and death. Illness usually occurs within 15 to 50 days after eating or drinking contaminated food or water. Symptoms include fatigue, nausea, vomiting, abdominal pain, and jaundice. Consumers who ate the potentially affected berries in the last two weeks and have not been vaccinated against hepatitis A should immediately consult with a physician, the FDA said. from https://ift.tt/FLMTKOQ Check out https://takiaisfobia.blogspot.com/ LONDON — The World Health Organization’s top monkeypox expert said she doesn’t expect the hundreds of cases reported to date to turn into another pandemic, but acknowledged there are still many unknowns about the disease, including how exactly it’s spreading and whether the suspension of mass smallpox immunization decades ago may somehow be speeding its transmission. In a public session on Monday, WHO’s Dr. Rosamund Lewis said it was critical to emphasize that the vast majority of cases being seen in dozens of countries globally are in gay, bisexual or men who have sex with men, so that scientists can further study the issue. She urged those at risk to be careful. “It’s very important to describe this because it appears to be an increase in a mode of transmission that may have been under-recognized in the past,” said Lewis. “At the moment, we are not concerned about a global pandemic,” she said. “We are concerned that individuals may acquire this infection through high-risk exposure if they don’t have the information they need to protect themselves.” She warned that anyone is at potential risk for the disease, regardless of their sexual orientation. Other experts have pointed out that it may be accidental that the disease was first picked up in gay and bisexual men, saying it could quickly spill over into other groups if it is not curbed. Read More: What Is Monkeypox and Should You Be Worried? Last week, WHO said 23 countries that haven’t previously had monkeypox have now reported more than 250 cases. On Monday, the U.K. announced another 71 monkeypox cases. Lewis said it’s unknown whether monkeypox is being transmitted by sex or just the close contact between people engaging in sexual activity and described the threat to the general population as “low.” Monkeypox is known to spread when there is close physical contact with an infected person, their clothing or bedsheets. She also warned that among the current cases, there is a higher proportion of people with lesions that are more concentrated in the genital region and sometimes nearly impossible to see. “You may have these lesions for two to four weeks (and) they may not be visible to others, but you may still be infectious,” she said. Last week, a top adviser to WHO said the monkeypox outbreak in Europe, U.S., Israel, Australia and beyond was likely linked to sex at two recent raves in Spain and Belgium. That marks a significant departure from the disease’s typical pattern of spread in central and western Africa, where people are mainly infected by animals like wild rodents and primates. 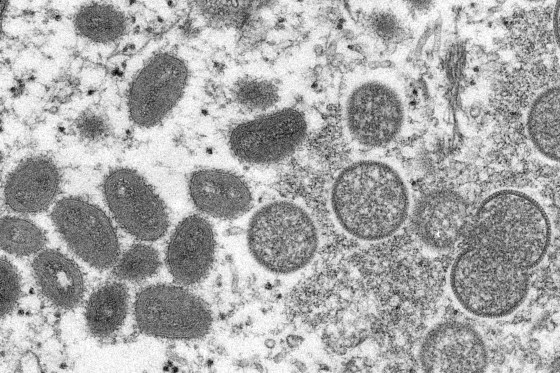
Monkeypox in AfricaScientists haven’t yet determined whether the monkeypox outbreak in rich countries can be traced to Africa, but the disease continues to sicken people on the continent. On Monday, authorities in Congo said nine people have died of monkeypox in 2022. Dr. Aime Alongo, chief of the Sankuru health division in Congo, also said 465 cases have been confirmed, making it one of the worst-hit nations in West and Central Africa. Nigerian authorities confirmed the country’s first monkeypox death this year, in addition to six more cases. WHO says thousands of cases are reported from Nigeria and Congo every year. Most monkeypox patients experience only fever, body aches, chills and fatigue. People with more serious illness may develop a rash and lesions on the face and hands that can spread to other parts of the body. No deaths have been reported in the current outbreak beyond Africa. WHO’s Lewis also said while previous cases of monkeypox in central and western Africa have been relatively contained, it was not clear if people could spread monkeypox without symptoms or if the disease might be airborne, like measles or COVID-19. Read More: There’s Already a Monkeypox Vaccine. Not Everyone May Need It Monkeypox is related to smallpox, but has milder symptoms. After smallpox was declared eradicated in 1980, countries suspended their mass immunization programs, a move that some experts believe may be helping monkeypox spread now, since there is now little widespread immunity to related diseases. Smallpox vaccines are also protective against monkeypox. Lewis said it was also uncertain how much immunity people who were previously vaccinated against smallpox might still have, since that was at least more than four decades ago. She said WHO’s priority was to stop the current spread of monkeypox before the disease became entrenched in new regions. “If we all react quickly and we all work together, we will be able to stop this,” she predicted. “We will be able to stop it before it reaches more vulnerable people and before it establishes itself as a replacement for smallpox.” --Chinedu Asadu in Abuja, Nigeria, contributed to this report from https://ift.tt/sNl0Lpw Check out https://takiaisfobia.blogspot.com/ For a few months in the fall of 2021, reports of unchecked violence, abuse, and neglect at the jail on New York City’s Rikers Island were plastered across national news before receding back into the routinized cruelty that constitutes the underbelly of American life. This exceptional coverage of the brutality behind bars provoked universal condemnation. But in its short-lived ascent to the forefront of political discussions and popular media, this media “event” failed to account for the most unsettling reality at play: Rikers is everywhere. Last week, while acknowledging that “people are dying” as a result of neglect at the jail, a federal judge nonetheless granted New York City Mayor Eric Adams more time to avoid Rikers being put into federal receivership—a threatened slap on the wrist for the city’s repeatedly fatal refusals to respect the constitutional rights of those it cages. As Rikers continues to be scrutinized, both national news media and federal authorities are largely ignoring that the conditions noted at Rikers are far closer to the norm than exception across U.S. carceral facilities. Abysmal conditions at Houston’s Harris County Jail, for example, drove even more deaths last year than at Rikers, and parallel sustained crises continue across the country. Over what has been by far the deadliest two years in their history, a large proportion of U.S. jails and prisons have demonstrated themselves incapable of fulfilling their legal obligations to ensure safe conditions for those they hold inside their walls. Even prior to the pandemic, all 50 states were reporting an inability to hire staff at adequate levels to ensure basic safety. This has worsened significantly since. Jail and prison administrators have responded by dramatically increasing their reliance on solitary confinement as a supposed “protective” measure, with the subjection of 80,000 people held in solitary on an average day in “normal times” ballooning to approximately 300,000 held in such conditions during the pandemic. When enforced more than 15 days, as has long been accepted as standard operating procedure in U.S. facilities, solitary is defined by the U.N. as torture and a blatant violation of human rights. Abusive conditions like these, alongside woefully (and illegally) deficient health care in jails and prisons, have led to substantial increases in suicides, homicides, ignored medical emergencies, general health care neglect, and COVID-19 outbreaks among incarcerated people. And, in the context of absent data and auditing systems alongside incentives to cover up abuse inside jails and prisons, however bad things may appear on paper, they are certain to be far worse in reality. Read more: COVID-19 Has Devastated the U.S. Prison and Jail Population In response, many officials have done what New York City is proposing for Rikers: close the most dysfunctional facilities while simply redistributing the people they hold. For example, at least 12 states have closed prisons over the last year in connection with staffing shortfalls and reports of systematic abuse, violence, and generalized disorder. Although this may appear to constitute wins for the prison-reform movement, these states have all refused to pair these closures with substantial reductions to the number of people they lock up. Without both releasing incarcerated people—beginning with the hundreds of thousands of people whose continued incarceration, data show, does not prevent violence and instead actually leads to increased crime—and addressing the front-end criminalization of poverty, officials are simply relocating and concentrating the problem of chronic overcrowding. Such piecemeal reforms detached from a vision and pragmatic plan for more transformative changes are exacerbating and prolonging untenable health and safety conditions in jails and prisons. Putting facilities like Rikers into federal receivership—that is, under the control of federal, rather than state or city, authorities—without addressing root causes is likely to do the same. Although this would allow federal actors to bypass current laws, local politicians, and correctional officers’ union contracts that are obstructing the jail from meeting its constitutional obligations, it would again sideline the fact that U.S. jails are harmful by design, not aberration. As legal scholar and criminologist Mark Findlay wrote four decades ago when mass incarceration was still in its infancy, “As long as prison reformers attempt to work within the existing correctional system to reform it, reform will be dissipated as the reformers inevitably are conditioned to accept the retention of the basic correctional structure in exchange for minor revisions.” What reformism ignores is that it is the intrinsic conditions of incarceration itself that harm the health and safety of incarcerated people, staff, and the public writ large. Consider, for example, that even before COVID-19 supercharged the harm inflicted by incarceration, one study estimated that an incarcerated person loses two years of future life for each year spent locked up; another study calculated roughly five years of life expectancy lost by age 40 alone. And these life-shortening consequences of incarceration also affect family members, communities, and, ultimately, the entire country. When one in three Black men in the U.S. are incarcerated during their lifetimes and men of all backgrounds face an 11% lifetime likelihood of incarceration, the sheer scale of harm inflicted by the U.S. punishment system is difficult to fathom. Read more: The True History of America’s Private Prison Industry The COVID-19 pandemic, by turning the long-standing violence of incarceration into a plague for us all, has put a long-repressed reality into stark relief. Conditions inside jails, prisons, and criminalized neighborhoods cannot be separated from the health of broader communities. As a consequence, lawmakers’ ostensible attempts to build public safety via shortsighted systems of segregation like incarceration are doomed to boomerang back as multiplying harm for everyone. Throughout the COVID-19 pandemic jails and prisons have operated as epidemic engines that multiply and spread disease throughout surrounding communities. My own research, for example, indicates that jail-related spread of the coronavirus has driven millions of COVID-19 cases and tens of thousands of deaths. This epidemiological dynamic long predates COVID-19 and, if we fail to make major changes, will continue long after the present pandemic has passed. The truth is the system of policing and incarceration that has been promoted as the centerpiece of U.S. “public safety” policy for the last half-century is, in reality, fundamentally incompatible with shared safety. This cannot be fixed through superficial bureaucratic rearrangements, such as hiring private contractors as short-term guards, bringing in the National Guard, using CARES Act funding to build yet more jails and prisons, further increasing funding for police, putting abusive facilities under the control of the federal government, or closing the worst jails or prisons only to shift incarcerated people from one harmful context to another. In defense of his proposed jail reforms and bid to retain city control of Rikers, Mayor Adams’ Corrections Department commissioner, Louis Molina, claims that “change must come from within” and not via external interventions. By contrast, advocates for abolitional justice like Angela Davis, Ruthie Wilson Gilmore, and Mariame Kaba emphasize that systems built on racist, violent premises cannot yield genuine solutions. As they point out, to suggest that we must place our trust in the U.S. carceral system to fix itself reflects, at best, profound naivete and historical ignorance. At the more realistic worst, it reflects a callous strategy used by those in power to hold onto their positions regardless of the human costs. To wake from our national carceral nightmare will require forcing large-scale decarceration upon unwilling system administrators, like Commissioner Molina and Mayor Adams and their counterparts nationwide. As endorsed in consensus expert recommendations for decarceration issued by both the National Academies and the American Public Health Association, this means investing in the release and reentry into society of approximately 1 million people whose ongoing confinement serves no plausible public interest. It also means investing in decriminalization, housing, and non-police public safety systems––like a national community health worker corps––in order to stop cycles of counterproductive arrests. Despite the overwhelming scientific evidence for the rational necessity of such action, however, politicians who fear appearing “soft on crime” have refused to take responsibility for implementing change. On the rare occasions in which carceral abuse garners significant media attention, policymakers—both Republicans and Democrats—along with judges, prosecutors, and prison officials typically respond by expressing shock, as if they had never before heard of the barbaric reality of these systems. Next, these public officials issue empty calls for incremental reform until the problem again fades from public view. Similarly, in a period of ongoing emergency inside jails and prisons, federal and local officials are repeatedly lamenting their supposed powerlessness while refusing to make use of the decarceration tools at their disposal. President Biden has failed to show leadership; instead, he is repeating what’s brought us to this point. And Congress has done no better, refusing to enact genuine public safety policies, such as those outlined under The BREATHE Act framework that reallocates funding from failed policing and prison models and redirects it towards supportive social services that are far more effective at preventing violence. When key pieces of such paradigm-shifting legislation—such as The People’s Response Act and The Counseling Not Criminalization in Schools Act—have been introduced, they’ve been largely ignored. Meanwhile, as mass shootings decimate yet more families and communities with each passing week, preventable death continues undeterred by either police or the specter of prisons. It’s long past time that we confront the absurdity of spending approximately $280 billion of taxpayer dollars on policing and punishment annually and another $768 billion for militaristic delusions of “national security” while hundreds of thousands of Americans are killed each year as a result of grossly deficient health, labor, and welfare systems that, in turn, fuel endless carceral loops. The fact is that there will be no possibility of safety in the U.S. until we abolish our indefensible carceral system and build in its place the public infrastructures required to reverse a half-century of persistent investments in cruelty rather than care. from https://ift.tt/AISmpx8 Check out https://takiaisfobia.blogspot.com/ The May 24 mass shooting in a Uvalde, Texas elementary school, in which a gunman killed 19 young children and two teachers, was the third-deadliest school shooting in U.S. history. But it was also just the latest of an increasingly common type of U.S. tragedy—one that experts say is saddling American schoolchildren, even the youngest, with rising levels of anxiety and other mental-health problems. Even when children aren’t directly involved in school shootings, they are deeply affected by them and often experience anxiety and depression as a result, says Kira Riehm, a postdoctoral fellow at the Columbia University Mailman School of Public Health. “These events are extremely high profile, and they’re portrayed hugely in the media,” says Riehm. They also happen with alarming frequency. In 2022 so far, there have already been 27 school shootings in which someone was injured or killed, according to Education Week’s school shooting tracker. In a study published in 2021 in JAMA, Riehm and other researchers surveyed more than 2,000 11th and 12th graders in Los Angeles about their fear of shootings and violence at their own or other schools. Researchers followed up with those same students and found that kids who were initially more concerned were more likely to meet the criteria for generalized anxiety disorder and panic disorder six months later—suggesting that kids internalize these fears, which can then manifest as diagnosable mental-health issues, Riehm says. While the researchers didn’t find an overall association between concern about school violence and the development of depression, they did when they looked specifically at Black children. “The root issue is this concern and fear that this could also happen at your school or another school,” Riehm says. “They are large numbers, and unfortunately, that’s kind of in line with what I would have expected before even looking at the data.” Children of all ages are at risk for developing these types of symptoms after shootings, but research shows that younger children are even more likely than older ones to develop symptoms like anxiety and PTSD as a result, says Dr. Aradhana Bela Sood, a professor of psychiatry and pediatrics at Virginia Commonwealth University. “Elementary school kids are probably going to have a much rougher time than perhaps older adolescents,” says Sood. Younger kids haven’t developed “those defenses, those capacities to sort things out in the brain,” Sood says. “They just haven’t had life experiences. And they have no idea how to make sense of this.” Read More: Close-Knit Uvalde Community Grieves After Elementary School Shooting In a 2021 review published in Current Psychiatry Reports, Sood and her colleagues analyzed research about the effects of mass shootings on the mental health of children and adolescents. They found that young children (ages 2 to 9) who are directly or indirectly exposed to violence have increased rates of PTSD, but, older children (ages 10-19) “need multiple exposures to violence—direct or indirect—for it to lead to PTSD, suggesting that younger children are more sensitive to violence and develop psychological symptoms post exposure to violence at a higher rate,” the study authors write. (In the review, direct exposures were defined broadly as witnessing or surviving a violent event; indirect exposures included seeing images of a shooting.) High social media use and continuous news reporting on mass shootings expose children repeatedly to these disturbing stories, which “can have at least short-term psychological effects on youth living outside of the affected communities such as increased fear and decreased perceived safety,” the authors write. Gun-related concern has been widespread among U.S. schoolkids for a long time. Shortly after the 1999 Columbine High School shooting in which 13 people were killed, researchers surveyed high school students across the U.S. Their results, published in the American Journal of Preventive Medicine, found that 30% more students said they felt unsafe at school, compared to national survey data collected before the shooting. This is evidence of “vicarious traumatization,” Sood says, which can occur when a child hears about a tragedy or sees images of it—even if they don’t experience it firsthand. Sood says that kind of exposure is much more likely to produce long-term damage in children who already have shown symptoms of anxiety and depression—which describes a growing number of American kids. “There are certain children that I would be very vigilant about,” Sood says. While young children are deeply affected by traumatic events, the good news is that they are also resilient. “Obviously there’s an impact, but what you want to see over weeks is a gradual reduction in this response, and that’s normative for young kids,” Sood says. Whether a child is directly or indirectly impacted by a mass shooting, there are specific steps parents and guardians can take to help their young children process the tragedy. “It is important for people around the child to be vigilant and aware of how they can be supportive and allow the evolution of the grief,” Sood says. Giving the child a predictable routine, allowing them to talk about the experience without judgment, and limiting the news that the child takes in about a tragic event all help, Sood says. Parents or guardians should also make sure they are taking care of their own mental health. The omnipresent threat of gun violence is just one of the many contributors to the worsening mental-health crisis among U.S. adolescents. Riehm says that issues like climate change and COVID-19 are other large concerns. In November 2021, the American Academy of Pediatrics, American Academy of Child and Adolescent Psychiatry, and Children’s Hospital Association jointly declared a national emergency for the mental health of children. “We are caring for young people with soaring rates of depression, anxiety, trauma, loneliness, and suicidality that will have lasting impacts on them, their families, and their communities,” the experts wrote. from https://ift.tt/u8hacRU Check out https://takiaisfobia.blogspot.com/ The U.S. is still in the throes of an unprecedented infant-formula shortage. Supply-chain issues caused by the pandemic started affecting baby formula in the summer of 2021, and inventory constricted even further after Abbott recalled certain formula products in February (then more in March) and shut down its Michigan plant. Families facing empty shelves are terrified that their children will go hungry, since breast milk or formula—or a combination of both—is a main source of nutrition for babies from birth until about age one. “It’s not fair that families have to be even worried about this on top of being a new parent,” says Dr. Shweta S. Namjoshi, medical director of intestinal rehabilitation and nutrition support at Stanford Children’s Health. “It’s unacceptable.” But pediatricians are experts on finding infant food, and they can help families locate shops where formula is in stock, safely guide them to different brands, and coach them through this stressful time. “I’m sorry that it feels so scary, but there’s no need for panic quite yet,” Namjoshi says. Here’s what pediatricians say about how to safely navigate the formula shortage. Try a different brandFor parents of full-term, healthy infants, it’s very safe to switch to different brands of infant formula, including generic versions. “The way formula is marketed makes it so that parents feel fear and pressure, like ‘Oh, I can’t switch brands,’… but that’s just not true,” Namjoshi says. Even when products say that they are formulated for certain issues—like anti-gas or anti-reflux—they will work just fine for most babies without diagnosed issues, she says. “Enfamil, Gerber—they’re all basically the same. They use the same mix of sugars, the same proteins, the same fats.” Children may be a little fussy as they go through an adjustment period with a new brand, but often “it’s just a child acclimating to something different,” she says. However, children with special needs and medical conditions—such as some immune-compromised children, those with allergies or gastrointestinal issues, and premature babies, for instance—may require specialized formulas, such as hypoallergenic or lactose-free formulations. These patients should work closely with their physicians when they explore new formula options. “For babies who are on typical formulas, they’re able to find something,” says Dr. Rachel Dawkins, medical director of the pediatric and adolescent medicine clinics at Johns Hopkins All Children’s Hospital. “But it’s those children with special health-care needs that might be on a specialized formula—they’re really having a struggle.” Because every type of formula is now so hard to find, some parents of healthy infants are buying specialized formulas, which are often the only options left on shelves. Infants without medical issues can safely use them, doctors say, but they should only do so if they are the only option left, because some babies can only use those specialized formulas. Take advantage of government optionsFamilies receiving formula from WIC—the national nutrition program for low-income women, infants, and children that serves nearly half of all infants in the U.S.—now have additional options. On May 21, President Joe Biden signed the Access to Baby Formula Act of 2022 so that WIC may offer more types and sizes of formula cans during emergencies like this. The U.S. is now importing formula from other countries as well, and the U.S. Food and Drug Administration (FDA) is looking to change its rules on allowing international shipments of formula during shortages. Several international companies “are seeking urgent approval for those types of formulas,” says Dr. Steven Abrams, professor of pediatrics at the University of Texas at Austin Dell Medical School and past chair of the nutrition committee at the American Academy of Pediatrics (AAP). He expects the FDA to grant rapid approval for international brands “in the next week or two.” “People are beginning to understand that the system didn’t have enough safety points,” Abrams says. “We need to have a lot more backup,” he says, and a system that doesn’t just rely on just a few companies to make nearly all of the country’s formula. Don’t hesitate to ask your pediatrician for helpIf you can’t find formula or are nervous about running out, or if your baby is fussy from trying different brands, your pediatrician can help guide you through this stressful time. Pediatricians can access backup supplies of formula—children’s hospitals still have formula, for instance, though that should be nobody’s first stop—and they are also closely attuned to where formula is in stock. Doctors can also offer advice and referrals to lactation support for families looking to start breastfeeding or increase supply. “Your baby’s going to be okay,” Namjoshi says. “No pediatrician will ever let your child just go hungry. We have backups.” Don’t replace formula or water it downCow’s milk and plant-based milk alternatives are not acceptable substitutes for breast milk or formula. These liquids are missing essential nutrients that babies need for proper nutrition and could cause health issues for infants. The U.S. Centers for Disease Control and Prevention (CDC) recommends introducing whole milk from cows around the first birthday. If infants drink too much of it before then, they could develop intestinal bleeding, kidney issues, and dairy allergies. Parents should also never water down formula in order to make the cans last longer. Doing so can cause hyponatremia, a condition that occurs when sodium levels drop too low, which can lead to seizures. Not getting enough nutrients can also lead to a failure to thrive. Making your own homemade formula is another bad idea, experts say. “There’s plenty of recipes and old wives’ tales out there, but they’re not safe,” Dawkins said. “They don’t supply the necessary nutrients for babies and may cause some electrolyte problems and nutritional deficiencies.” Be cautious when obtaining formula or breast milk that’s not from a store“It’s okay to crowdsource in your local communities or on different mommy groups online, but I would just make sure that the cans of formula aren’t expired and they’re not open,” Dawkins says. “Sometimes people have extra, and I think it’s great to be able to help out your neighbor.” But be wary of sharing breast milk from a freezer stash. “What we would prefer is for people who have extra milk to donate it to their milk banks,” Abrams says. The banks screen milk donors for health conditions, pasteurize the milk, and distribute it to the babies who need it most—often those in neonatal intensive care units. Informal milk sharing networks aren’t regulated the same way milk banks are, and the milk could be adulterated or unsafe. “We have to be cautious about direct milk sharing or wet nursing, and especially cautious about anything from a donor you don’t personally know,” Abrams says. Don’t panic-buyIt might be tempting to fill your pantry with formula if you’re able to find it, but it’s important to leave some on the shelves for other families who need it. “Don’t worry excessively if you have plenty of supply,” Dawkins says. “Hopefully the end is in sight for the formula shortage.” from https://ift.tt/97uXJor Check out https://takiaisfobia.blogspot.com/ It’s impossible to quantify the cost of gun violence. There’s no way to add up pain and grief. No way to multiply that by shock and outrage. But emotional suffering and physical injuries do become real numbers when traumatic shooting events, like other public-health epidemics, contribute to the national health care burden. A 2021 review of hospital costs from the Government Accountability Office revealed about 33,000 inpatient stays and about 51,000 emergency room visits every year to treat firearm injuries. Those initial hospital visits were nearly triple the average patient cost, and collectively topped $1 billion annually. More than half of the cost was for patients with Medicaid and other public coverage. For gun-wound survivors and their families, there’s a hefty price tag affixed to the healing process following a shooting incident, according to a Harvard Medical School study published in April that analyzed Medicare and commercial insurance claims between 2008 and 2018. Compared with their peers, gunshot survivors had a 40% increase in pain diagnoses, a 51% increase in psychiatric disorders, and an 85% increase in substance-use disorders in the aftermath of the shooting. Their family members had a 12% increase in psychiatric disorders. Among injured survivors in the study, medical spending topped $25,000 per person one month after the shooting. Over 12 months, the costs totaled about $30,000 per survivor—or approximately $2.5 billion when multiplied by the 85,000 people who survive firearm wounds every year in the U.S., the study found. The costs were linked to treating survivors’ physical injuries and also subsequent mental health conditions in the first year following the shooting. Gunshot survivors included in the study all had insurance coverage, and so didn’t pay out of pocket for all those expenses. Still, the study found that their co-pays and deductibles combined went up about $100 per month, on average, in the first year. What’s more, that financial burden didn’t account for lost productivity, wages, or employment (which could impact their ability to pay for health care), nor did it account for longer-term rehabilitation costs in later years. For survivors’ significant others, parents, and children, medical spending was nearly $80 higher per person in the first month after the injury, but not statistically different over a one-year period. However, the study didn’t account for the population of families that lost a loved one to gun violence, nor the financial hardships associated with caring for a gunshot victim. Another analysis from Everytown Research, a gun safety advocacy organization, puts medical costs even higher than the Harvard study, at $3.5 billion a year, though that figure accounts for survivors’ long-term care, coroner services for fatally shot victims (of which there are some 40,000 a year), and mental-health services for family members. The Everytown analysis notes that, beyond the direct medical and health costs, the overall financial toll of gun violence on American society is hundreds of billions of dollars, including quality-of-life costs that are inherently intangible, but can be loosely estimated based on jury awards and victim settlements. In the wake of high-profile mass shootings, like the most recent shootings at a Buffalo, N.Y. supermarket and a Uvalde, Texas elementary school, there’s often a flurry of fundraisers to support the affected families and communities. Some instances of gun violence result in remuneration following lawsuits. Such financial buffers—that is, the ones that no one ever wishes for—don’t bring down the costs that the broader health care system has to shoulder. Nor do they relieve the personal and collective sorrow that the U.S. has endured time, and time, and time again. from https://ift.tt/qsmBvwR Check out https://takiaisfobia.blogspot.com/ Dr. David Ho has spent his entire career studying HIV and other viruses, so he thought he knew what to expect when he recently became infected with SARS-CoV-2. His symptoms weren’t very severe, but after discussing it with his doctor, Ho decided to take Paxlovid, the antiviral COVID-19 therapy made by Pfizer, for the five-day course. At 69, he fit the description of someone who should. The U.S. Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) recommend Paxlovid for people at higher risk of severe COVID-19, including seniors. Ho carefully tracked his infection. He had access to PCR testing and genetic sequencing in his lab at Columbia University, as well as rapid antigen kits for self-testing at home. He started taking Paxlovid a day after he first experienced cold symptoms and an antigen test turned positive. A PCR test on day 2 confirmed the infection, and Ho continued taking the daily therapy of two different pills for five days, as indicated. Every day from day 4 to day 9, his antigen tests were negative, and two PCR tests performed on day 5 and day 7 were also negative. But on day 10, he had a headache, runny nose, and mild cough. Ho decided to test himself at home, and to his surprise, he was again positive, which a PCR test confirmed. His team sequenced the virus to compare it to the genetic sequence from his earlier infection and found that it was identical to the virus that he had been infected with days before—suggesting that the virus hadn’t mutated to become resistant to Paxlovid, nor had he become infected again with a different virus. The same infection had come roaring back after being quelled for a few days. “I was surprised to see the rebound,” he says. “I was expecting Paxlovid to take care of things.” A rebound like Ho’s was always a known potential side effect of the drug. In studies, Pfizer reported that 1% to 2% of people taking the medication experienced rebound. The company says the rates of rebound in the treated group in its study and among those receiving placebo were similar, indicating that “elevated nasal viral RNA is uncommon and not uniquely associated with treatment.” But a growing number of people are reporting infection rebounds after taking Paxlovid—so many that “there’s no way it’s occurring at 1% or 2%,” says Ho, who has also shared his data and discussed it with scientists at Pfizer. “It’s happening quite a bit.” Anecdotes from people who test positive, take a course of Paxlovid, test negative, and then days later test positive again abound on social media. It’s been scientifically documented; researchers at the University of California, San Diego recently described one case of rebound in a May 18 paper published on the pre-print server Research Square (which means it has not yet been peer reviewed). And on May 24, the CDC issued a health advisory instructing doctors caring for patients who take the drug about how to manage rebound cases. Ho decided to study the phenomenon further when he learned that a colleague, Dr. Michael Charness at the VA Boston Healthcare System, had a similar experience. The scientists (who are both vaccinated and boosted) teamed up and conducted what is probably the most comprehensive analysis of the phenomenon to date, because they were able to conduct daily testing and track the flip from negative to positive and also perform genetic sequencing of the virus to confirm that the infection was caused by the same virus rebounding back, rather than a new infection. Their paper, published on Research Square, describes their own cases, as well as eight additional ones in which people reported rebounding virus after taking Paxlovid. Here’s what we know about Paxlovid rebound so far. Why do people even take Paxlovid if their COVID-19 could rebound?Paxlovid is a combination of two drugs: a protease inhibitor used to treat HIV infections that blocks the virus from making critical proteins it needs to replicate, and another that prevents the liver from breaking down the drug too quickly in the body. It’s not currently FDA approved, but doctors can prescribe it under an emergency use authorization. The authorization was based on studies conducted by Pfizer that showed the drug was up to 88% effective in protecting unvaccinated people from needing hospitalization for COVID-19, or from dying of the infection. The company is continuing to study Paxlovid in those who are vaccinated and boosted to see if their immune responses somehow react differently to the drug. In a statement to TIME, a Pfizer spokesperson said “We are continuing to monitor the data, but we have not seen any resistance emerge to date in patients treated with Paxlovid. We believe the return of elevated detected nasal viral RNA is uncommon and not uniquely associated with treatment. We remain very confident in Paxlovid’s clinical effectiveness at preventing severe outcomes from COVID-19 in high-risk patients.” Why does Paxlovid rebound happen?Scientists are still trying to determine why people with COVID-19 are taking Paxlovid, testing negative for several days, and then testing positive again. But they are exploring several potential reasons. One hypothesis is that people are simply getting infected again in quick succession with different variants of SARS-CoV-2, since cases are mounting in the country and because the virus is mutating so quickly. Another explanation might be that because the virus mutates so rapidly, it has developed a way to escape Paxlovid and become resistant to its effects. But Ho believes something else is going on. His small study showed that three of the infections in his report—his, Charness’, and that of one other person—were rebounds of the first, not new strains or a new Paxlovid-resistant variant. Based on the genetic sequencing data, “we showed the rebounding virus is not resistant to the protease inhibitor [drug in Paxlovid], because there is no change in protease sequence,” he says. “It’s not reinfection with another virus. The sequences are identical.” Pfizer says its studies similarly showed that the virus is not developing resistance to the protease inhibitor drug. Instead, Ho believes the virus is just doing what viruses do in response to antiviral medications. No antiviral drugs—whether against SARS-CoV-2 or HIV—actually kill any virus present in an infected person; they work by blocking certain steps in the virus’ replication cycle, freezing them in time so the virus cannot continue to churn out more copies of itself. Paxlovid specifically interrupts the step involving the protease enzyme, which splices the long string of polypeptides that the virus makes once it infects a cell. That lengthy protein needs to be cut into its component proteins, which then play roles in making a new virus. By inhibiting that step, Paxlovid leaves the virus in a suspended state—and depending on when the drug was started, an infected person could have thousands of these long polypeptide strings already made and floating around in the body, creating a latent reservoir of viral product that could become active again. The drug prevents these intermediary forms from getting cut and infecting cells, but once the drug stops after day 5, the enzyme is no longer inhibited and can go back to splicing and making viral proteins. That could lead to a rebound, because more virus is being made that can infect cells again. “We know the drug has a very short half life, which means it doesn’t linger for long in the body,” says Ho. “The virus hasn’t been killed by the drug, but only blocks its replication. There is still a reservoir of viral material, so for a virologist, that’s the first thing we think of. Once the drug is washed out, that reservoir can become active again.” Ho is currently doing experiments in his lab to figure out how long the intermediary polypeptide of SARS-CoV-2 can remain in the body, in order to determine whether the 5-day treatment window is long enough. It’s possible that one way to minimize rebound infections is to extend the number of days people take Paxlovid, but Pfizer would have to conduct new studies to determine how many additional days would be needed, and how safe and effective the drug would be if that were the case. Pfizer is considering whether to conduct these studies in order to better understand if specific populations might need longer treatment with the medication. Should you take Paxlovid again if you test positive after finishing the 5-day course?According to the CDC’s recent health advisory on Paxlovid rebound, the agency does not recommend that people who have finished the five-day course restart taking the pills. Instead, the CDC advises people who test positive again to restart a five-day period of isolation and to wear masks for 10 days after rebound symptoms begin. Ho says the CDC reached out to discuss best strategies for managing rebound prior to issuing the new guidance. The CDC does not specifically recommend that people on Paxlovid test themselves more regularly after finishing their treatment, but Ho advises that people follow current advice and run a rapid at-home test if any symptoms, however mild, reappear, regardless of whether they have taken Paxlovid or not. How sick will I get if I test positive again after taking Paxlovid?The CDC notes that most people who rebound experience mild symptoms the second time, and most will recover without the need for additional treatment. If I test positive after taking Paxlovid, am I still contagious?Yes. Anyone who tests positive on a rapid test—even after finishing a full course of the drug treatment—is again contagious and can pass the virus on to others. It’s important for people taking Paxlovid to be on the lookout for the possibility of a rebound infection and use rapid at-home antigen tests as often as they can, and confirm the diagnosis with a PCR test if possible, so they will know if they turn positive again. In the 10 cases in Ho’s report, two people transmitted the virus to others in their household after they had relapsed. “The idea of somebody who goes virus-negative and then could become virus-positive again—that’s of great concern,” he says. Given the possibility of a rebound, is it worth taking Paxlovid?The emergency use authorization currently restricts doctors to prescribing the drug only to people at higher risk of developing serious disease, which includes older people and those with compromised immune systems. Otherwise healthy people, especially those who are vaccinated and boosted, may not benefit from the therapy, especially since people need to start taking it as close to when they first experience symptoms as possible in order for it to be effective. The rebound might just extend quarantine periods for them as well, since they might recover without the drug and not experience rebound infections in a shorter period of time. from https://ift.tt/FxDtbdr Check out https://takiaisfobia.blogspot.com/ New U.S. research on Long COVID-19 provides fresh evidence that it can happen even after breakthrough infections in vaccinated people, and that older adults face higher risks for the long-term effects. In a study of veterans published Wednesday, about one-third who had breakthrough infections showed signs of Long COVID. A separate report from the Centers for Disease Control and Prevention found that up to a year after an initial coronavirus infection, 1 in 4 adults aged 65 and older had at least one potential Long COVID health problem, compared with 1 in 5 younger adults. [time-brightcove not-tgx=”true”] Long COVID refers to any of more than two dozens symptoms that linger, recur or first appear at least one month after a coronavirus infection. These can affect all parts of the body and may include fatigue, shortness of breath, brain fog, and blood clots. Coronavirus vaccines that help prevent initial infections and serious illnesses provide some protection against Long COVID but mounting research shows not as much as scientists had first hoped. The veterans study published in Nature Medicine reviewed medical records of mostly white male veterans, aged 60, on average. Of the 13 million veterans, almost 3 million had been vaccinated last year, through October. Read More: At Least 20% of People Who Get COVID-19 Develop Lingering Conditions, CDC Study Says About 1%, or nearly 34,000, developed breakthrough infections. Lead author Dr. Ziyad Al-Aly noted that the study was done before the highly contagious Omicron variant appeared at the end of the year and said the rate of breakthrough infections has likely increased. Breakthrough infections and Long COVID symptoms were more common among those who had received Johnson & Johnson’s single-dose shot compared with two doses of either Moderna or Pfizer vaccines. Whether any had received booster shots is not known; the first booster wasn’t OK’d in the U.S. until late September. Overall, 32% had Long COVID symptoms up to six months after breakthrough infections. That’s compared with 36% of unvaccinated veterans who had been infected and developed Long COVID. Vaccination reduced the chances for any Long COVID symptoms by a “modest” 15%,” although it cut the risk in half for lingering respiratory or clotting problems, said Al-Aly, a researcher with Washington University and the Veterans Affairs health system in St. Louis. These symptoms included persistent shortness of breath or cough and blood clots in lungs or veins in the legs. Infectious disease expert Dr. Kristin Englund, who runs a center for Long COVID patients at the Cleveland Clinic, said the Nature Medicine study mirrors what she sees at her clinic. Long COVID patients there include people who were vaccinated and received boosters. “As we have no clear treatments for Long COVID, it is important for everyone to get vaccinated and use other proven methods of prevention such as masking and social distancing in order to prevent infections with COVID and thus Long COVID,’’ Englund said. The CDC report, released Tuesday, used medical records for almost 2 million U.S. adults from the start of the pandemic in March 2020 to last November. They included 353,000 who had COVID-19. Patients were tracked for up to a year to determine if they developed any of 26 health conditions that have been attributed to Long COVID. Those who had COVID were much more likely than other adults without COVID to develop at least one of these conditions, and risks were greatest for those aged 65 and older. Information on vaccination, sex and race was not included. Breathing problems and muscle aches were among the most common conditions. Older adults’ risks were higher for certain conditions, including strokes, brain fog, kidney failure, and mental health problems. The findings are worrisome because those conditions can hasten older adults’ needs for long-term care, the report authors said. They stressed that routine assessment of all COVID patients “is critical to reduce the incidence” of Long COVID. from https://ift.tt/PhLs8Wf Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
