|
It’s time for my healthy nine-year-old son to get vaccinated against COVID-19. In fact, it’s time for every kid aged five to eleven to get vaccinated. An advisory committee to the Food and Drug Administration (FDA) has reviewed the data from clinical trials assessing the safety and efficacy of the Pfizer-BioNTech vaccine in children five to eleven years old. The experts voted unanimously to recommend authorization for this vaccine in children in that age range. As a next step, the Centers for Disease Control and Prevention (CDC) will decide whether all kids should have access to the vaccine, or only some. Some experts have proposed use in high-risk children only while we accumulate additional data. Waiting to vaccinate all children would be a mistake. Based on the data we have, the right answer is clear: the CDC should recommend that all kids ages five to eleven should have be vaccinated as quickly as possible. There is one thing all experts agree on: Vaccinating children should be based on rigorous evidence and we should set a particularly high bar for using vaccines in healthy children. The Pfizer COVID vaccine has cleared that bar. Whether these vaccines work in kids is beyond dispute: they are extremely effective, reducing COVID infections by more than 90 percent. This number is based on data gathered during the Delta surge in the U.S., when vaccine breakthroughs among adults were becoming more common in the U.S. Such a high level of protection from the vaccine at a time when infection rates were extremely high is remarkable. A common source of confusion, sewn largely by COVID-19 minimizers, is around whether we should be vaccinating kids because children are less likely to get sick than adults. This is true—but also not the point. The real question is how the risk of COVID in kids compares to other risks children face. Here, the data for protecting kids is compelling: COVID-19 was the sixth-leading cause of death among children ages five to eleven in 2020 and overall, has led to nearly 700 deaths among children. In a typical flu season, approximately 200 children die, an unacceptably high number for which we recommend universal vaccination. COVID remains far more deadly for children than the flu. The next question is how the risks and benefits of the vaccine compare to the risks of getting COVID. Here, the calculation is also straightforward: the virus is a constant threat, to our children and all with whom they interact—including playmates, friends, and relatives. We have seen what COVID can do if we don’t control its spread. The worst of the Delta surge is behind us, but over 1000 Americans still die every day from the disease. Vaccines prevent infections and the spread of the virus, and save lives. Like all vaccines, COVID vaccines can have the standard side-effects of a sore arm, fever or headaches, but these side-effects are mild and short-lived. There are also important concerns about one specific side effect that is crucial to recognize and fully understand: myocarditis—or an inflammation of the heart muscle. Myocarditis in the pre-COVID era was a rare condition more commonly associated with infections from viruses such as influenza or coxsackie. These cases could occasionally be serious leading to long-term complications due to direct infection of the heart muscle by the virus itself or the intense immunologic response triggered by the infection. We see this myocarditis in unvaccinated children who have been infected by COVID, where some cases can be serious. Vaccine-induced myocarditis is quite different. First, it is very rare. In fact, we know that the risk of getting myocarditis from COVID among 12- to 17-year-olds, for whom we have the best data, is about 1 per ten thousand children vaccinated. The side-effect occurs more often in boys, as often as 17 per 100,000 boys vaccinated. We don’t know why this difference exists, though there may be a role for the hormone testosterone. But these rare instances of vaccine-related myocarditis cases in teenagers were mild and the teens recovered in a week or two. For children 5 to 11, no cases of myocarditis were detected in clinical trials. The trial included 2,000 children who received the vaccine so it is possible very rare side-effects could be missed. But it is clear that myocarditis is not a common side effect in five- to eleven-year-olds, and that the rates of myocarditis in this population of largely pre-pubescent children, particularly boys, is likely to be even lower than in teenagers. We need to start preparing for a world in which SARS-CoV2 will be endemic, circulating for decades or longer, just like measles, whooping cough and the flu. I care about my child’s health over the long term, not just the brief window when side effects may occur. The benefits of vaccination, even if there is some waning, will last years. Beyond 6 months after vaccination, the risk of side-effects from a COVID vaccine is essentially zero. The benefits for my child will be substantial. This is why essentially every expert on child health has come out in support of vaccinations. The American Association of Pediatrics, has been vocally supportive, as has the American Association of Family Practitioners, who represent physicians who care for millions of children. I get it. Kids don’t like any vaccines. Needles are scary. My 9-year-old has asked if there is an option that doesn’t involve a needle. I wish there was. And, of course, for a parent, it can seem scary to you to give your child a new vaccine. We want to do the right thing, in frighteningly unfamiliar circumstances. It is helpful to take a step back, and remember how vaccines have transformed our lives, and the life expectancy of our children. We give children dozens of vaccines, without which they would be vulnerable to potentially fatal diseases from measles to pneumococcal disease—diseases that continue to sicken unvaccinated children around the world. It is time for the CDC to continue its important work on protecting our children by adding another tool to the arsenal. We need COVID vaccinations for all children five to eleven years old so parents can get their children vaccinated and keep them safe. That’s what I’m going to do. from https://ift.tt/3pPH3Ug Check out https://takiaisfobia.blogspot.com/
0 Comments
These days, there’s a lot to be anxious about. Between losing loved ones and experiencing financial strain to family stress and fears about illness, many of us are struggling more than ever. In a 2021 survey of more than 3,000 adults, 47% reported feeling anxious, and 57% of Black adults said they worried about their future. In addition, 54% of essential workers admitted to drinking alcohol and overeating to ease their emotional pain. Anyone who’s experienced anxiety knows the distress it can bring. Often, this spiky emotion causes a racing heart, headache and knotted stomach. Frequently, we interpret these sensations as a danger sign. For instance, we might mistake social anxiety as evidence that everyone dislikes us or believe performance anxiety means we’re actually impostors. While anxiety certainly feels terrible, it does have an upside. In her new book, Good Anxiety, neuroscientist Wendy Suzuki repositions anxiety as a potentially positive force in our lives that can open the door to self-care and resilience—two things that inoculate us from stress. From this vantage point, social jitters might be a sign to reach out for support, while performance woes might be a signal to practice our craft a little more or spend two minutes in a power pose. When we realize anxiety can be a helpful messenger, we can make it work in ways that benefit our psychological well-being. From this perspective, anxiety isn’t a symptom we solely manage with medication or behavioral therapies (even though research shows these treatments work); it’s also a cue to search for its underlying cause. Like a detective, we can start by asking ourselves some exploratory questions. For instance, “How does anxiety show up in the body?” “What is it telling us?” and “What core emotions brew beneath our anxiety?” Illuminating anxiety’s relationship to underlying core emotions can lead to lasting change, emotion-focused researchers point out. Core emotions like sadness, anger, fear, disgust, joy, excitement and sexual excitement affect the whole body to make it move in ways that help us survive and thrive. This is why fear mobilizes the body for running and anger gets us ready to fight. However, we also have another category of emotions called inhibitory emotions, more commonly known as anxiety, guilt and shame. The key to moving through anxiety lies in understanding the difference between core and inhibitory emotions. As emotion-focused therapists and educators, we teach our patients about this relationship. Like a high-speed motor, anxiety revs us up, making it hard to think clearly because our thoughts and feelings become a threat. When we’re in this amped-up state, anxiety blocks core emotions, making it impossible to sense our emotional needs, let alone use them in ways that help us. The good news, however, is that we don’t need to remain stuck. Anxiety can be a clue that we need to identify and experience our core emotions, which leads to calm and clarity. Here are some tools that can help untangle anxiety and make it work in our favor, not just in the moment but for years to come. Acknowledge anxiety. When children are flooded with big feelings, adults often tell them to “use their words,” because putting language on anxiety helps dial it down. Researchers call this “affect labeling.” One study found that naming negative emotions calmed down the amygdala, the part of the brain where feelings light up. When this happens, emotional reactivity loses its charge because the right and left parts of the brain become more connected, says psychiatrist and author Dr. Dan Siegel in his book Mindsight. For instance, many of our patients tell us they obsess over their mistakes or ruminate about work, which are common symptoms of anxiety. In situations like these, merely saying to yourself, “I feel anxious” can lead to what psychologist Diana Fosha, developer of Accelerated Experiential Dynamic Psychotherapy. calls a “click of recognition.” Naming our emotional experience is validating, which permits us to be authentic. In addition, accepting our emotions disarms the need for defense mechanisms—behaviors like overworking, denial and addiction that numb pain but suck up vital energy. Without the need for these Band-Aids, we’re better equipped to use our energy to engage in work and relationships. Slow anxiety down. When you’re anxious, a decisive step is to slow the body down with body-based tools like grounding and deep belly breathing. When we’re in the throes of anxiety, being told to “take a deep breath” can come across as overly simple or downright aggravating. However, science tells us breathing can slow down anxiety’s engine. Neuroscientist Steven Porges, who developed “polyvagal theory,” says diaphragmatic breathing stimulates the vagus nerve, which triggers the body’s relaxation response. When this happens, stress hormones like cortisol decrease, and we feel immediate relief, say researchers. When a patient tells us they’re worry-filled, we invite them to slow down their nervous system by saying, “Right now, can you give yourself permission to move away from your thoughts and into your body? Bring your attention to the soles of your feet as they meet the floor. Sense the firm ground underneath you.” Next comes the invitation to shift into deep belly breathing. We teach, “Take the deepest breath you can and send the air down to the base of your abdomen. Let your belly pop out like a Buddha and try to keep your chest down.” We suggest placing one hand on the chest and the other on the belly to help with this process. Then, we teach them to hold their breath for one beat, then slowly release the breath through pursed lips like they’re blowing on hot soup. We coach them to tune into their body during the whole breathing cycle so they can learn how to breathe in a maximally relaxing way. Get curious about core emotions. According to Dr. Judson Brewer, a physician and scientist, curiosity can be anxiety’s companion. Defined as the “desire to take in new information,” curiosity can open the mind to possibilities, which helps us search for novel solutions. Researcher Jordan Litman calls this “interest curiosity,” and studies show it can increase motivation and enhance learning. Thus, through curiosity’s lens, we can see anxiety as an invitation to identify our underlying core emotions. To do this, we encourage our patients to adopt a compassionate and non-judgmental stance toward themselves. Then, we invite them to scan their body from head to toe and notice where they feel anxiety. Next, we ask them to imagine moving the anxiety aside so they can notice what core emotions they are feeling. For example: “Is sadness there?” “Is anger there?” “Is excitement there?” More than one core emotion may be present, and they can be opposite. For instance, we can feel sadness and anger at the same time. Noticing each core emotion can help us listen to the message they’re sending. Anxiety always has a more profound meaning. It’s never the end of the story; it’s the beginning. Identify the conflict. Anxiety can be a symptom of a deep inner conflict that’s throwing us into torturous thinking. For instance, a patient may want to go home for the holidays but dread being with their parents, which causes them to ruminate and feel tense. To get out of this bind, it helps to validate each side of the conflict, or as we say in our practice, change the “but.” Doing so negates each opposing side to an “and,” which creates room for both feelings to coexist. For example, we can validate our desire to see our family, and honor the anger that their hurtful behaviors evoke. Then we can come up with solutions to deal with their behaviors—such as setting boundaries, which can include saying things like, “Dad, if you continue calling me names, I’ll leave.” Sadly, our dysfunctional society, with its many antiquated myths about emotions, sends the message that anxiety is pathological or a genetic defect. But emotion education tools can turn this frightening foe into a wonderful teacher. In the end, anxiety isn’t a sign of weakness. It’s a sign of being human. from https://ift.tt/3BsBn4G Check out https://takiaisfobia.blogspot.com/ A version of this article also appeared in the It’s Not Just You newsletter. Sign up here to get a new edition every weekend. It’s easy to careen through the day, barely conscious of our transactions large and small. Pay for a coffee with a wave of your phone, order a week’s groceries by voice command. And if a disaster has hit the news, you can donate money and sprinkle supportive emojis across social, just tap, tap, tap. This is the age of insta-generosity, insta-consumption, insta-everything. And that’s not entirely a bad thing. We can raise vast amounts of aid in hours with the same tools we use to make sneakers appear on our doorstep. But in both cases, we’re scarily removed from the people on the other side of our screens. And that gulf between us has never been more acute than now as we live more of our lives remotely. Addressing this disconnect was a priority when mindfulness teacher and community activist Shelly Tygielski created a grassroots mutual aid organization called Pandemic of Love in March of 2020, just as the coronavirus was bearing down on her South Florida neighborhood. As she writes in her new book, “Sit Down to Rise Up: How Radical Self-Care Can Change the World,” the concept was to match donors directly with those in need ensuring that there’d be an interaction between giver and receiver. “What I’m proudest of is the fact that I purposely built Pandemic of Love to be sure that human beings could connect at a time of isolation,” says Shelly. “We could have taken money on behalf of people and then just distributed it, which is fine. But I knew that we all needed human interaction as much as anything else.” 
A year and a half later, the organization has become a global phenomenon, connecting almost two million people who’ve shown up for each other and been changed by the experience. And in a year of many heroes, Shelly was named one of CNN’s 2020 Heroes of the Year, not just because of the $60 million in aid that Pandemic of Love has facilitated, but because of the unique way the group uses social media and technology to spark person-to-person connections. “It’s not just giving financial assistance or supplies,” says Shelly. It’s that you’re making someone feel seen and letting them know that they’re not alone. And the people on the donor side also feel seen from these interactions.” These very personal transactions are not without vulnerability, both for those who are asking for help from a stranger, and the givers who are opening themselves to another’s life and struggle. Clearly, there’s a yearning for this kind of connection. Thousands of Pandemic of Love volunteers are matching people across the world to provide everything from diapers for a single mom to rent money. This kind of mutual aid addresses our other pandemic, that of toxic division. The book includes uplifting stories in which Pandemic of Love donors and recipients crossed political and cultural barriers to see each other differently. (We’ve showcased some of these case studies in this newsletter. And below, you’ll find the tale of two women who connected, much to their own surprise: Eileen, a self-described New York hippy liberal, and Christine, a single mom from Mobile, Alabama.) The other argument Shelly makes is that self-care and community care are not in opposition; they’re entwined. “The successful inner journey of me leads towards a collective healing of we,” she writes. It was a lesson she discovered as a single mother dealing with a newly diagnosed health condition. She’d hit a wall and admitted to a few close friends that she couldn’t handle what was on her plate. Those friends became a tiny mutual aid group, meeting to share their to-do lists and, most importantly, their self-care plans. They supported each other, offering help, like covering school pickups, and they kept each other accountable for the kind of self-care that fosters resilience, like prioritizing sleep. Shelly expanded this grassroots safety net to a wider array of acquaintances and found that when one person raised their hand and said, “I need help,” a door opened for everyone. “In emergencies like when there’s a death or a hurricane, everyone steps up,” says Shelly. “But we need to normalize that kind of community care even when there isn’t a disaster. Social media isn’t going to show you what might be happening on your street. You don’t know if your neighbor is struggling with mental illness or if they just lost their job because we just don’t talk about it. We need to create forums for these conversations.” Sign up here to get an essay from Susanna Schrobsdorff every weekend. When I ask Shelly how to create a community of care if we aren’t as organized as she is, she points out that she didn’t intend to create a huge aid organization. Her original goal was just to make sure the people in her community had enough to make it through the pandemic. She says:
But why not just focus on your own well-being and your immediate family, if you feel depleted? “We can’t survive without each other,” says Shelly. “Our grandparents and great grandparent’s generation knew this. And it’s still true. Look at the supply chain issues that are happening right now. Or the first responders and front-line workers we relied upon over the last year.” Shelly offers a short meditation as a way of reminding ourselves that we don’t exist in a bubble. Whenever she buys something, even a tomato, she tries to stop and think about the provenance of that item. “Consider the thousands of hands that touched that tomato in some way—those who tended the earth, planted the seeds, and packed the boxes,” she says. “And all millions who inspired and cared for those people. It’s a beautiful meditative exercise to just pause for a moment of reflection and think about that as often as you can during the day. It’s humbling.” You might call it heart training, this decision to visualize the bonds that connect us to the world, and to each other. At the very least, it’s a bid for awe over anger. Sign up here to get an essay from Susanna Schrobsdorff every weekend. THE ROUND-UP ?For More On Building Community: Check out this TEDTalk, Inspiring a life of immersion. We each want to live a life of purpose, but where to start? In this luminous, wide-ranging talk, Jacqueline Novogratz introduces us to people who have immersed themselves in a cause, a community, a passion for justice. How to Fend Off Winter Depression: As the days get shorter and the nights start earlier, take these steps to help prevent seasonal affective disorder. People Aren’t Meant to Talk This Much: A lot is wrong with the internet, but much of it boils down to this one problem: We are all constantly talking to one another. Is there a case to be made for scaling back and opting for fewer, deeper ties? “How to Learn Everything: The MasterClass Diaries”. Irina Dumitrescu, an essayist and professor of medieval English literature, binged for six months on online courses led by celebrities like RuPaul, Anna Wintour, and Gordon Ramsay. Her piece on MasterClass is a delightful take on the power of celebrity and learning new things. (This piece was included in this year’s The Best American Essays” collection.) EVIDENCE OF HUMAN KINDNESS ❤️Here’s a reminder that creating a community of generosity elevates us all. And this week, we’re republishing a story from Pandemic of Love that shows how giving can help us cultural divides. Eileen is a self-described liberal, feminist, hippie-New Yorker. A retired social worker, she worked primarily with the LBGTQIA+ and immigrant populations. In early April, she was matched by Pandemic of Love with a single mother named Christine in Mobile, Alabama, who needed help. Eileen describes the initial shock of the connection as one between “two very different people from two very different worlds.” When Eileen found out that she had voted for President Trump in the last election and planned to vote for him again, her initial instinct was to ask if she could be re-assigned to another family. Christine had the same thought at the start, “to be honest; I didn’t think I was going to like her when we met. She is a New Yorker, and I am just a Southern girl at heart.” But the pair decided to move forward. And since July, Eileen has been sending Christine and her family bi-weekly help for groceries and essentials, and upon learning that Christine’s 8-year old daughter loves to read, she started to send her books. “I honestly do not know what I would have done without her all this time,” says Christine. The two unlikely friends speak and text frequently and have talked about everything from the Holocaust to the Confederate Army. Christine is certain she and Eileen will be friends for life. And while Eileen began the relationship thinking Christine was living in a red-state bubble, she says she’s shocked to realize “how long I have been living in a bubble, too.” Story courtesy of Shelly Tygielski, author of “Sit Down to Rise Up” and founder of Pandemic of Love, a grassroots mutual aid organization that matches volunteers, donors, and those in need. Write to me at: [email protected], or via Instagram: @SusannaSchrobs. And, sign up here to get a new edition of It’s Not Just You every weekend. from https://ift.tt/3mpDC4K Check out https://takiaisfobia.blogspot.com/ (LONDON) —Pharmaceutical company Merck agreed to allow other drug makers to produce its COVID-19 pill, in a move aimed at helping millions of people in poorer countries get access to the potentially life-saving drug, a United Nations-backed public health organization said on Wednesday. The Medicines Patent Pool said in a statement that it had signed a voluntary licensing agreement for molnupiravir with Merck and its partner Ridgeback Biotherapeutics. The agreement will allow the Medicines Patent Pool to grant further licenses to qualified companies who are approved to make the drug. Neither drug maker will receive royalties under the agreement for as long as the World Health Organization deems COVID-19 to be global emergency. Molnupiravir is the first pill that has been shown to treat the disease. Charles Gore, the executive director of the Medicines Patent Pool, said the early results for molnupiravir were “compelling” and that he hoped this first voluntary licensing agreement for a COVID-19 treatment would lead to others. Despite repeated requests from governments and health officials, no vaccine makers have agreed to a similar deal. A hub set up by WHO in South Africa intended to share messenger RNA vaccine recipes and technologies has not enticed a single pharmaceutical to join. Merck has requested its pill be licensed by both the U.S. Food and Drug Administration and the European Medicines Agency, decisions that could come within weeks. Merck reported this month that molnupiravir cut hospitalizations and deaths by half among patients with early symptoms of COVID-19. The results were so strong that independent medical experts monitoring the trial recommended stopping it early. An antiviral pill that people could take at home to reduce their symptoms and speed recovery could prove groundbreaking, easing the crushing caseload on hospitals and helping to curb outbreaks in poorer countries with weak health care systems. It would also bolster a two-pronged approach to the pandemic: treatment by way of medication and prevention, primarily through vaccinations. The charity Doctors Without Borders welcomed the agreement Merck struck to share its COVID-19 pill, but said it didn’t go far enough. “The license excludes key upper-middle-income countries like Brazil and China from its territory, where there are strong, established capacity to produce and supply antiviral medicines,” said Yuanqiong Hu, a senior legal and policy adviser at Doctors Without Borders, who called the deal “disappointing.” from https://ift.tt/3BjwKdh Check out https://takiaisfobia.blogspot.com/ COVID-19 vaccines are already authorized for children ages 12 and older, and the shots now have the support of a U.S. Food and Drug Administration (FDA) expert panel for younger children ages 5 to 11. In a 17 to 0 vote, with one abstention, the committee recommended the COVID-19 vaccine made by Pfizer-BioNTech for the youngest group yet to potentially get immunized against the disease in the US. The committee recommended a two-dose regimen at one-third the dosage approved for adults. The FDA now takes the committee’s advice into consideration before making a final recommendation. If the agency decides to recommend the vaccine, the Centers for Disease Control and Prevention (CDC) will then detail which specific groups of children in that age range should get vaccinated. (For example, after weighing the benefits of risks, the agency’s public health experts could recommend only children at high risk of severe COVID-19 get the shot.) That was a question the FDA committee members struggled with as well, since the data presented by Pfizer-BioNTech included balancing the benefit of the vaccine in protecting kids from COVID-19 disease against theoretical risks of side effects, nearly all of which have been observed in older children and adults. Those complications include inflammation of the heart tissue, which is known as myocarditis and pericarditis. The committee members also grappled with the fact that, according to data presented by CDC scientists, up to 40% of children aged 5 to 11 may have already been infected with SARS-CoV-2, and that may be an under estimate, since many younger children who are infected don’t experience symptoms and therefore never go to the doctor or get medical care. That means they might have some immunity against the virus, although it’s unclear how robust it would be. “I think it’s possible they likely only need one dose at best, which is going to be more than sufficient for them,” said Dr. Michael Kurilla, director of the division of clinical innovation at the National Institutes of Health, who abstained from the vote. Kurilla expressed concern that Pfizer-BioNTech did not provide data detailing what happens to the virus-fighting antibodies that children generate after getting vaccinated, and whether these wane as they do in adults. He also worried about vaccinating children who might have already been naturally infected and not need additional protection from a shot. The U.S. is reviewing data on how safe and effective each of the three authorized or approved COVID-19 vaccines is for children. On Oct. 25, Moderna submitted its request to the FDA to expand its authorization to include children ages 6 to 11. That was based on data the company provided showing that the vaccine can provide strong protection against COVID-19 disease. For today’s discussion, Pfizer-BioNTech provided data from two studies involving more than 3,100 children ages 5 to 11 who received either two doses of their vaccine or two doses of a placebo. About half were tracked for two months or more, and half for under a month. According to Pfizer-BioNTech’s studies, the two shots, each given at one-third of the dosage for adults, were 90.7% efficacious in protecting the children from getting symptoms of COVID-19. Three children who got the vaccine tested positive for COVID-19, while 16 in the placebo group tested positive seven days after their second dose. The committee agreed that children with underlying health conditions, including obesity and chronic diseases like diabetes, would benefit from vaccination. But for otherwise healthy children, the balance wasn’t as clear—given, as Kurilla noted, the relatively high proportion of children who might already have immunity from natural infection, as well as the potential risk of myocarditis. In older adolescents and adults, the heart risk was rare but concerning, especially among young males, and the vaccine’s label currently contains a warning for this group. But it’s not clear if the same risk translates to younger children. That’s why the FDA asked Pfizer-BioNTech to provide additional data on more than 1,500 youngsters, in addition to the original 1,500 that the companies originally studied, which allowed the agency to delve more deeply into the side effects. In its analysis, the FDA noted that people who are naturally infected with COVID-19 have a nearly 16-fold increase in the risk of myocarditis compared to those who are not infected. The scientists also weighed the risk of Multisystem Inflammatory Syndrome (MIS-C), a rare condition that causes fever, loss of blood pressure and damage to different organs including the liver. Over the past year, the CDC recorded more than 5,200 cases of MIS-C and 46 deaths, mostly in children ages 5 to 13 years. The FDA scientists did extensive modeling to predict how the benefits and risks would play out, and found that the balance was highly dependent on how much virus is circulating. During peak infections, the benefits of protecting children from the disease outweigh the small risks of complications from the vaccine, but in one model, which assumed very low prevalence of COVID-19 in the community, the risk of myocarditis, estimated from rates occurring among older children, offset any potential benefit of the vaccine. Still, overall the FDA concluded that the potential longer term risks of COVID-19 infection, including Long COVID, may tip the balance in favor of vaccination. “To me, the question is pretty clear. We don’t want children dying of COVID-19 even if there are far fewer children than adults affected by the disease, and we don’t want them in the ICU,” said Dr. Amanda Cohn, chief medical officer at the National Center for Immunizations and Respiratory Diseases at the CDC. Ultimately, the FDA committee’s role is to evaluate the safety and efficacy of the vaccine for a specific age group. It’s up to the CDC to decide exactly which children in that age range should get vaccinated. That swayed most of the committee members to vote in favor, ensuring that children who need the vaccine and could benefit from it can get vaccinated if their parents so choose. “I voted ‘yes’ because I want to make sure that children who really need this vaccine—mainly Black and brown children—get the vaccine,” said Dr. James Hildreth, professor of internal medicine at Meharry Medical College. “There are lots and lots of children for whom the vaccine could be the difference between health and even life. I hope the [CDC’s committee] will prioritize the vaccine in some way to make sure that actually happens.” Dr. Eric Rubin, editor in chief of the New England Journal of Medicine and professor of immunology at the Harvard T. H. Chan School of Public Health and Brigham and Women’s Hospital, admitted that “we decided to vote for it with a heavy conscience. I’m hoping this is the start of learning more about how to deploy this vaccine.” Children, and especially younger children, are the last group to be vaccinated against COVID-19, following the elderly, adults and adolescents. As more people in the U.S. have been vaccinated, rates of new infections have declined, along with hospitalizations and deaths from the disease. But infections and disease are climbing among the youngest children, highlighting the need to vaccinate them quickly. Of the more than 44 million cases of COVID-19 reported since the pandemic began, nearly 9% have occurred among children aged 5 to 11 years. In August, 39% of cases among people under age 18 were in 5 to 11 year olds. Nearly 150 children in this age group have died of COVID-19. Even more concerning, young children may be getting infected without symptoms and spreading the virus to others. Dr. Anthony Fauci, chief medical advisor to the White House and director of the National Institute of Allergy and Infectious Diseases, said at a recent briefing that “months ago, it was felt, based on the data with [the] Alpha [variant] predominantly, that children do not get infected as much. And if they do, they don’t spread the infection in the home setting. In the era of Delta, children get infected as readily as adults do, and they transmit the infection as readily as adults do.” That means that as more adults are vaccinated, the virus is finding new hosts to infect to survive—such as young, unvaccinated kids who are serving as sources of infection to other children (as evidenced by the outbreaks among summer camps last year), as well as unvaccinated and immunocompromised adults. “The reality is that at one point we thought if we vaccinated enough people, then the virus would go away,” said Jeannette Lee, professor of biostatistics at the University of Arkansas. “But it’s not going away, so we have to find a way to live with it. Vaccines give us a way to do that.” from https://ift.tt/3pBLzpn Check out https://takiaisfobia.blogspot.com/ When Americans divide themselves into camps, they stick to them fiercely: Democrats versus Republicans, pro-life versus pro-choice, gun rights versus gun control. Add to that, as has become apparent over the course of the past year, those who are pro- versus anti-coronavirus vaccines. As with so many other polarizing issues, your position on getting or not getting inoculated against COVID-19 has become more than a medical question. It’s morphed into a form of cultural identifier, a sign of your membership in one tribe or another. More than ever, that’s becoming clear as booster shots are rolled out around the nation, with about 70 million Americans now eligible for an additional dose and tens of millions more set to join them as the eligibility age inevitably falls. The extra dose comes as very good news to a lot of the population—people who are mindful of the way vaccine-induced antibody levels fall over time and anxious to bump them back up. But that doesn’t remotely include everybody, with resistance to even initial vaccinations keeping the country far from the much hoped-for herd immunity. All of this is playing out as the government looks beyond first doses and encourages Americans to step up for their extra dose. Plenty of people are responding. According to data from the U.S. Centers for Disease Control and Prevention (CDC), booster rates are now exceeding first-shot rates across the country. In the week ending October 24, just over 400,000 people per day were getting boosters, compared to just over 200,000 receiving their first shots. 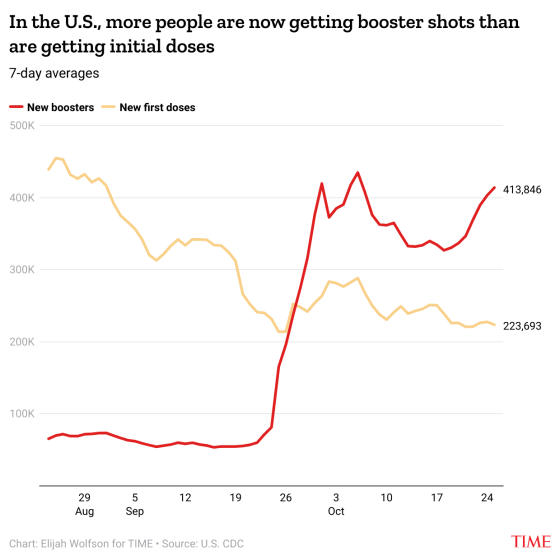
Those numbers have been moving in a sort of Newtonian, equal-and-opposite dance since late August, when more than 400,000 people daily were getting first doses and boosters were just being rolled out to the immunocompromised. The lines crossed in late September, when the CDC recommended Pfizer-BioNTech boosters for at-risk groups, and the upward trend for boosters and downward trend for first shots has continued since. Boosters got another bump on October 21, when the CDC approved additional doses of the Moderna and J&J vaccines. Those recommendations, CDC director Rochelle Walensky said in a statement last week, “are another example of our fundamental commitment to protect as many people as possible from COVID-19.” When it comes to the boosters, the government’s pro-vaccine message is apparently being heard. When it comes to first doses, not so much. This story was adapted from The Coronavirus Brief, TIME’s daily COVID-19 newsletter. Sign up here. from https://ift.tt/3mj1VRS Check out https://takiaisfobia.blogspot.com/ Most guidelines and data on breast cancer have come from studies of white women of European descent. “I don’t experience the screening recommendations in the same way that white women do,” says Yvette Gullatt, chief diversity officer for the University of California system. “I experience breast cancer in Black women as highly aggressive and lethal. I’ve had white colleagues who were diagnosed with breast cancer and go to radiation in the morning, and are back at work by 10 a.m.; they never miss a day.” Gullatt joined the WISDOM study, which stands for Women Informed to Screen Depending On Measures of risk, in the hopes that she can improve breast cancer care for Black women. “We need more studies like this because [researchers] need more data in order to diagnose and treat us better,” she says. The WISDOM study was launched in 2016 by Dr. Laura Esserman with the hope of bringing a more personalized approach to figuring out each woman’s risk for the disease, plus tailor a screening and treatment program appropriate for that risk. Esserman and her team are working closely with community advocates to increase awareness and education about clinical trials among Black women, who already have a deep mistrust of the medical system given notorious episodes of medical exploitation, including the Tuskeegee and Henrietta Lacks experiences. In those cases, Black patients were used in research studies without being fully informed of their participation or the potential risks of participating. Providing them with the opportunity to learn more about research trials is especially important, since about 25% of breast cancers among Black women are triple negative, a highly aggressive form that’s missing the locks to three hormone-based drug “keys” that have become effective weapons in fighting the disease in recent years. Without these locks, the drugs can’t work, and tumors grow more quickly and seed new growths in other parts of the body. Most of these cancers also start in younger Black women, under age 40, so they aren’t picked up because they aren’t getting mammograms yet, per current guidelines. Rickie Fairley, a former marketing executive and breast cancer survivor, is working to improve education among Black women about the need to participate in trials like WISDOM. She has mobilized other women to serve as a clearinghouse for those who aren’t as familiar with the facts about breast cancer risk among Black women or about research and clinical trials. “Right now, we are not empowering Black women, or women of color, to understand the importance of research,” she says, noting that many Black women are afraid to join research studies. “There’s not enough data about Black women. We’re trying to figure out how to change the language so that we’re not afraid anymore, so that we take the fear away from any kind of research and empower us to participate in it.” As part of WISDOM’s recruitment, Esserman has also reached out to the VA health system in the U.S. to include female veterans whose risk of breast cancer may be related to not just hereditary factors but environmental exposures during their service. Lisa Edwards, a veteran who was discharged from the Army in 1989, says the study is an opportunity to raise awareness and resources for women’s health in the VA system in general. “As female veterans, we faced chemicals and exposure just as the men did,” she says. “But because our bodies react differently, I think in the future it may help researchers understand certain cancers from chemicals that react differently in women than in men.” Esserman hopes that having a more tailored approach to figuring out a woman’s risk based on her biological and social situation will mean that more women get the screening schedule and treatment for managing their breast health that’s right for them. from https://ift.tt/3pIcMXo Check out https://takiaisfobia.blogspot.com/ Moderna’s COVID-19 vaccine is safe and efficacious for children ages 6 to 11 years old who recieve two half doses, the company said today. That’s based on the results of its KidCOVE study, which involved more than 4,700 kids in that age group. The children participating in Moderna’s trial were randomly assigned to receive two half doses of the vaccine or two shots of a placebo. Those who got the vaccine generated adequate virus-fighting antibodies that met the U.S. Food and Drug Administration’s (FDA) requirements for efficacy, and the vaccine produced an immune response in nearly all the children. Most of the side effects after vaccination were mild to moderate, including fatigue, fever, headache and pain at the injection site. Meanwhile, an independent FDA panel will review data on the Pfizer-BioNTech vaccine in children ages 5 to 11 on Oct. 26. The age range in KidCOVE varies slightly, given that Pfizer-BioNTech included children as young as 5. Moderna is continuing to study younger children and will report results on kids ages 2 to 5 and 6 months to under 2 years in the coming months. The FDA and Centers for Disease Control and Prevention recently authorized a half dose of Moderna’s vaccine as a booster for certain adults over 18 years old. from https://ift.tt/3GjXKgr Check out https://takiaisfobia.blogspot.com/ (TAIPEI, Taiwan) — Children as young as 3 will start receiving COVID-19 vaccines in China, where 76% of the population has been fully vaccinated and authorities are maintaining a zero-tolerance policy toward outbreaks. Local city and provincial level governments in at least five provinces issued notices in recent days announcing that children ages 3-11 will be required to get their vaccinations. The expansion of the vaccination campaign comes as parts of China take new clampdown measures to try to stamp out small outbreaks. Gansu, a northwestern province heavily dependent on tourism, closed all tourist sites Monday after finding new COVID-19 cases. Residents in parts of Inner Mongolia have been ordered to stay indoors due to an outbreak there. The National Health Commission reported 35 new cases of local transmission had been detected over the past 24 hours, four of them in Gansu. Another 19 cases were found in the Inner Mongolia region, with others scattered around the country. China has employed lockdowns, quarantines and compulsory testing for the virus throughout the pandemic and has largely stamped out cases of local infection while fully vaccinating 1.07 billion people in its population of 1.4 billion. In particular, the government is concerned about the spread of the more contagious delta variant by travelers and about having a largely vaccinated public ahead of the Beijing Olympics in February. Overseas spectators already have been banned from the Games, and participants will have to stay in a bubble separating them from people outside. China’s most widely used vaccines, from Sinopharm and Sinovac, have shown efficacy in preventing severe disease and transmission of the virus, based on public data. But the protection they offer against the delta variant has not been answered definitively, although officials say they remain protective. Hubei, Fujian and Hainan provinces all issued provincial level notices alerting new vaccination requirements, while individual cities in Zhejiang province and Hunan province have also issued similar announcements. China in June had approved two vaccines — Sinopharm’s from the Beijing Institute of Biological Products and Sinovac — for children age 3-17, but it has only been vaccinating those 12 and older. In August, regulators approved another, Sinopharm’s from the Wuhan Institute of Biological Products. After the vaccines received domestic approval for children in China, foreign governments began giving the shots to children in their own countries. Cambodia uses both Sinovac and Sinopharm’s shots in children 6-11. Regulators in Chile approved Sinovac for children as young as 6. In Argentina, regulators approved the Sinopharm vaccine for children as young as age 3. Many developing countries left out of the race to get shots from Western pharmaceutical companies like Pfizer and Moderna bought Chinese vaccines. China has shipped more than 1.2 billion doses as of September, according to its Ministry of Foreign Affairs. Even with widespread domestic and global use, not every parent is reassured about the vaccine, citing less publicly available data on the shots. Wang Lu, who lives in the southern city of Fuzhou in Fujian province, said she isn’t particularly rushing to get her 3-year-old son vaccinated. “I’m just not very clear on the vaccine’s safety profile, so I don’t really want to get him vaccinated, at the very least, I don’t want to be the first,” Wang said. Sinovac started an efficacy trial with 14,000 child participants across multiple countries in September. Its approval in China was based on smaller phase 1 and phase 2 trials. Sinopharm’s Beijing shot was also approved based on smaller phase 1 and phase 2 trials. These were published later in peer-reviewed journals. Other parents said they weren’t concerned, given that many other people had already gotten the shot. Wu Cong, a mom of a 7-year old, said her daughter’s school in Shanghai hadn’t yet notified them of any vaccinations. “I think this isn’t too different from the flu vaccine, there’s already been so many people vaccinated, so I don’t have too many worries,” said Wu. Associated Press researcher Chen Si in Shanghai contributed to this report. from https://ift.tt/3jzSMlM Check out https://takiaisfobia.blogspot.com/ On a morning Zoom call, a group of Canadian mothers give their full attention to a young man from the Drug User Liberation Front. At 26, Jeremy Kalicum is the age some of their kids would be if they had not died of accidental overdoses. <strong>“We’re just sick of it. We’re sick of our friends dying.”</strong>Kalicum’s tone is urgent as he walks the moms through a PowerPoint presentation explaining why the Liberation Front, known as DULF, wants to protest on International Overdose Awareness Day and hand out illicit drugs. These wouldn’t be the kind that killed their sons and daughters, he assures them; they’d be “safe supply” drugs that have been tested to ensure they’re not laced with lethal fentanyl. “Anyone who wants to find drugs can find drugs,” says Kalicum, reasoning that the best way to save lives is to make sure users are given the safest possible drugs. “The drugs that they’re finding are of unknown quality and unknown potency.” Then, after 15 minutes of slides and stats, Kalicum and DULF co founder Eris Nyx makes their pitch: they want these mothers, from a group called Moms Stop the Harm, to join them and other activists in their distribution mission, an admittedly risky protest that could land them in jail. It’s a tough sell, but it’s critical to saving lives, say Kalicum and supporters of the “safe supply” effort. “I’m not a criminal, and obviously, Moms Stop the Harm aren’t criminals,” Kalicum says. “We’re just sick of it. We’re sick of our friends dying.” Everyone on the call can relate. Each has lost someone to the opioid crisis, which has soared in North America during the pandemic, especially in Canada. In the U.S., deaths rose nearly 30 percent in 2020 to a record 93,000. In Canada, deaths soared 89% over the previous year. 
Behind the numbers lies a cruel irony that every parent listening to Kalicum understands, and that drives the “safe supply” movement: Opioids were perfectly legal when their children were becoming addicted to them, promoted by pharmaceutical giants and doled out by physicians who enabled the crisis by accepting drug companies’ claims they were safe. When the reality became clear, and prescriptions became hard to come by, it was too late. Untold thousands of pain-addled patients had become hooked on what opioids provided, as had many young people who’d begun experimenting with the pills recreationally. They found relief on the streets in the form of heroin, then began dying from illicit drugs either laced with fentanyl or entirely replaced with the compound, which is 50 times more potent than heroin. A Deadly ArcThat is the arc of the Opioid Crisis: From patient to criminal to, more and more often, early death. The “safe supply” movement seeks to counter this deadly progression by ensuring the integrity of the dosages that users have been conditioned to crave while providing care that keeps them alive and could wean them off drugs. “It’s not who we are to stand passively by,” says Kalicum. “We’re gonna do something, and we’re willing to take on personal risks to do that. But we can look at ourselves in the mirror and know that we’re doing what’s right.” 
Even in Vancouver, a city with a progressive history on the issue of drugs, “doing what’s right” means butting up against an opposing force that still views drugs as a moral failing rather than a medical problem, and that opposes safe distributions. Slowly, though, DULF and the Vancouver Area Network of Drug Users, or VANDU, are drawing attention to their effort and, on this video call winning support. At least two of the moms listening to Kalicum volunteered to distribute drugs on International Overdose Day, Aug. 31, despite the risk of arrest. “If we lose some members, that’s okay,” says Leslie McBain, a founding member of Moms Stop The Harm. Her son died in 2014 just as lawsuits against opioid maker Purdue Pharma were first ramping up, and many were still naive to the dangers of opioids. “He had an injury on a construction site when he was 23, and the doctor just prescribed loads and loads of oxycodone,” she says of her son. “And that was his demise.” Read more: Inside the Worst Opioid Addiction Crisis in U.S. History In the past six years, McBain’s organization has grown to nearly 3,000 members across Canada. Their goal, she says, is to lessen the stigma of addiction and advocate for changes in drug policy in a way that “actually supports the lives of people who use drugs rather than punishes them.” In 2003, North America’s first sanctioned, supervised safe injection site, Insite, opened in Vancouver after receiving a federal exemption to protect it from the country’s drug laws. Canada now has 37 such sites, with zero overdose deaths at these supervised locations. In the U.S., cities with large communities of drug users like Boston, Seattle, San Francisco, and New York have tried to open safe injection sites, but none has done so legally. As a result, organizations working to help the most volatile drug users often operate in the shadows without official local or federal support. 
<strong>“History has shown that moving these initiatives forward often takes some form of civil disobedience from community groups.”</strong> Kalicum and Nyx are familiar with the pitfalls of trying to operate under the radar, having spent years on the front lines of the drug scourge. And as the pandemic’s effect on drug use has become clearer, with fentanyl showing up not just in heroin now but in cocaine and methamphetamine, the pair have become bolder in their efforts. They staged their first protest demanding a “safe supply” of drugs in 2020. In April 2021, they distributed “safe” heroin they tested for the first time in downtown Vancouver. Three months later, they distributed drugs in front of police department headquarters. ‘Maybe this is a good idea’“History has shown that moving these initiatives forward often takes some form of civil disobedience from community groups,” says Kalicum. The first overdose prevention sites were set up illegally along with needle exchanges. “It took people giving needles out themselves before the government thought maybe this is a good idea,” he says. The duo is a study in contrasts. Nyx, 30, is a witty, self-identified trans woman covered in tattoos, while Kalicum is more straight-laced, subdued, and serious. “I look like a criminal,” jokes Nyx. “Jeremy looks like he could be your best friend’s son.” 
<strong>“The thing about drugs is most people use them at least at some point.”</strong> But both bring a history of experience with drugs to their activism. Nyx is originally from the suburbs of Toronto. The organizing director of the Tenant Overdose Response Organizers and executive director of the Coalition of Peers Dismantling the Drug War; she says she’s used drugs since the age of 12 or 13, is estranged from her family for being queer and trans, and in turn experienced housing instability. In 2019, after being laid off from the British Columbia Center for Disease Control, Nyx was hired to organize a conference on “safe supply.” She and Kalicum met in person for the first time at that conference after weeks of planning calls, bonded over their shared mission, and created DULF. Kalicum was raised by a single mother on disability in the port city of Nanaimo, where he says his family was in “great need,” and he fell into drugs and petty crime at a young age. Eventually, a local charity put him through school in a suburb of Chicago until he moved back to Canada to complete his bachelor’s degree in chemistry and biology. Read more: A Community In Crisis His experience with that charity helped steer Kalicum into his current activism, which includes buying drugs on the dark web and testing them for evidence of fentanyl before they’re distributed as part of the “safe supply” movement. “That organization met people where they’re at and worked to improve their lives without any expectation of return,” he says. “And that’s what I strive to put forward into the world.” Much of DULF’s work focuses on “harm reduction,” which historically involves providing clean needles to prevent the spread of infection and disease, along with antiseptics, condoms, and anything else that might help safeguard drug users. It’s been shown to improve health outcomes that often lead to recovery. Long-term studies in Vancouver have shown that drug users were more likely to enter a detox program and save taxpayers money. In the early ‘90s, when Switzerland was dealing with a growing heroin epidemic, it began making methadone available. It launched a heroin prescription program for some users in an effort to curb overdose deaths, HIV infections, and public drug use. As these programs have grown, the rate of new heroin users has declined along with overdose deaths, HIV rates, and crime. Other countries, including the Netherlands, Denmark, Germany, the United Kingdom, and Canada, launched similar programs. 
Kalicum’s return to Nainaimo in 2016 coincided with the declaration of the opioid crisis as a public health emergency. He was shocked by the number of deaths in his home city and got in touch with a city councilor advocating for supervised drug consumption sites. Kalicum worked to set one up in Nanaimo, on Vancouver Island, and remembers, “that’s when I learned the value of direct action.” After moving across the strait to Vancouver in 2019, he became involved with the BC-Yukon Association of Drug War Survivors, an agency that advocates on behalf of drug users, and fell under the mentorship of Ann Livingston, considered a pioneer in harm reduction. Kalicum began to see it as his “moral imperative” to work around the legal system to save lives. Around that time, he also learned of “compassion clubs,” first used by terminally ill people to access cannabis for pain before it was legal. These clubs now provide drug users with a safe supply of drugs and with spaces in which people can supervise one another while using them. 
His arrival in Vancouver, as drug deaths were soaring, shook Kalicum. “Before I came to Vancouver, I’d never seen a dead body before,” he says. “And that summer, I’d seen several.” Currently almost six people die each day in British Columbia, according to the B.C. Coroners Service. Nyx says she responds to at least an overdose a week. “That f–ks a person up and creates an incredible amount of PTSD,” she says. Nyx and Kalicum know that they can’t wipe out drug use, but neither do they see that as something that should be done. “The thing about drugs is most people use them at least at some point,” Nyx says, citing coffee, cigarettes, alcohol, marijuana and prescription meds. Most people, she notes, use these substances and are not out of control or in what is often called “chaotic” use. “I don’t want to die. I’m a perfectly functional member of society, and most people who use drugs are,” she says. Read more: A Mother on the Pain of Losing Her Son to Opioids What would make more sense than focusing on the minority of out-of-control, self-destructive addicts, Nyx argues, is to regulate the drug market in a way that ensures all users have the safest options possible. Outlawing alcohol provides an instructive example. The Prohibition Era lasted only from 1920-23, but in that time the crime of drinking was driven underground into speakeasies and basements. Booze was mixed in buckets and bathtubs, and there were no labels on bottles. People had no idea what proof the liquor they were drinking was, and that was dangerous. Today’s illegal drug markets operate in the same way. No one has any idea what they’re buying on the street in unmarked bags. “Regulation will save people’s lives,” Nyx says. With that in mind, DULF has set out to do with street drugs what’s now common for alcohol and cigarette manufacturers: test ingredients and put clear labels on everything. The “DULF Fulfillment Center and Compassion Club model” acts as a market and consumer protection agency where street drugs are tested and distributed in packaging that states the drugs’ contents. 
Nyx, designs the labels, and together they promote the mission and crowdsource money to buy illegal drugs, then test them and distribute them at protests to people who are part of already existing drug-user groups. “The free drugs go to the people in the most need,” says Nyx. The Dark WebKalicum describes the system of buying drugs on the dark web, which is remarkably similar to buying just about anything else. “There are sites which are kind of analogous to eBay,” he says, where people can buy, and people can leave reviews for vendors. “These sites will hold your money in escrow until you get your product. When you get it, you test it. You can either release the funds or create a dispute,” he says. In the case of a dispute, the website appoints a mediator to settle things. DULF has received fentanyl instead of heroin and has been refunded thousands of dollars after creating a dispute. Still, there are unknowns, which has been one of the major criticisms of DULF: The seller might be a criminal organization, for instance. But Kalicum says the current state of drug legislation has left people serious about quality control no choice. “It’s not what we want to do,” says Kalicum, “but we’re forced to leverage the resources that we have access to, and that’s the dark web.” They pay for the drugs with a private cryptocurrency called Monero that claims to be untraceable. Kalicum was one of the first people hired to begin testing street drugs while working as a technician with the British Columbia Center on Substance Use, where he learned a technology called FTIR spectroscopy. The technology uses infrared light to tell him what’s in a substance and in what quantity. His goal eventually is to be able to use mass spectrometry, which shows a more refined level of detail. Nyx keeps track of the data on the drugs they distribute. Each person receiving a dose is asked to answer three simple questions on a form: did you use the drugs yourself, did the person using the drugs overdose, and will you score the drugs on a scale of 1 to 5? So far, Nyx says, of the 907 forms filled out, none of the users has overdosed. In this early phase, they don’t think that data can be leveraged in any official capacity, but Kalicum says, “it might act as a kind of carrot for researchers to do something substantial.” Kalicum would like to see heroin and other drugs provided by the government or a regulated supplier, the way methadone is now, and not by the illicit markets. “You’d be taking money out of the hands of organized crime,” says Kalicum. “People can get their drugs there, use them, and it acts as a portal to health and social services.” In May 2021, Vancouver offered up its own solution to the drug issue: the Vancouver Model, which would decriminalize simple possession of all drugs up to a specific amount. It recognizes substance use and the overdose crisis as a public health issue, not a criminal justice issue. Even so, DULF and many activists feel the proposal fails to address the sourcing of toxic drugs as the main cause of fatalities and that the amounts individuals would be permitted to possess don’t conform to actual patterns of substance use. Vancouver’s Police Inspector, Phil Heard, who took a leading role in proposing the plan, acknowledges the criticism but says it’s up to scientists, not cops, to study its impacts, assuming the idea is implemented. In the meantime, DULF is pushing hard to get permission to implement its own plan. In August, it submitted a 19-page letter to Canadian health officials asking for an exemption to practice its “safe supply” model. “We are saying this is a health emergency,” says Kalicum. DULF isn’t alone in what some consider radical approaches to the drug issue. As the pandemic raged through Canada in 2020, Canadian Health Minister Patty Hajdu, seeing the impact on drug users, raised the idea of injectable pharmaceutical-grade heroin, among other possible solutions.

Signs of progressIn August, Nyx and Kalicum presented their model to Inspector Heard and Staff Sergeant Jason Chan. The Aug. 31 protest marking International Overdose Awareness Day went smoothly, and none of the moms who took part was arrested. DULF has also received a “letter of support” for its testing and safe supply plan from Vancouver Coastal Health, a regional health authority with a budget of more than $3 billion dollars. Several Canadian policy experts, have also signed on, including many from the B.C. Centre on Substance Use and the Canadian Drug Policy Coalition. And on Oct. 7, the Vancouver City Council voted to support DULF’s plan, though it only passed after an amendment to ensure that drugs would be purchased through legal means. That would require activist groups to work with companies like Fair Price Pharma to supply, test, and package legally sourced drugs before dispensing them to members of a compassion club. Kalicum and Nyx addressed the meeting and urged officials to act quickly. then sort out the details of where to find drugs. “What we’re saying is a temporary stopgap. But stop the deaths first, then figure everything out after,” Nyx said. 
Everyone witnessing the overdose epidemic agrees that it is only getting worse. Heard, the police inspector says 2020 was a “record year,” but “2021, it’s looking to be even more deadly.” Sure enough, the day after the City Council hearing, Nyx witnessed yet another drug death, this time of an 18-year-old. Even with growing support, she and Kalicum are exhausted. They’ll need to apply for grants to fund their effort. “We have a colossal amount of work to do,” she says wearily. “People are constantly dying, and there is no end in sight.” from https://ift.tt/3B6IFLv Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
