Nationwide Protests Havent Caused a COVID-19 Spike (So Far.) Heres What We Can Learn From That6/30/2020 The coronavirus situation in the U.S. is bleak. While states like New York and New Jersey successfully turned the tide, others, like Texas and Arizona, are dealing with worsening outbreaks. At the national level, daily cases are rising daily, well exceeding the previous peak set earlier this year. And even in those few states that have gotten a grip on the pandemic, leaders are rethinking their reopening plans for fear of a relapse. But public health officials have spotted at least one bright spot amid all the discouraging data: the nationwide Black Lives Matter protests, which began after George Floyd’s death at the hands of Minneapolis police in May, so far do not seem to have been dreaded “superspreader” events, as some feared they might. Several cities that saw major protests, including New York, Chicago, and Philadelphia, have not experienced a new surge in cases in the days and weeks following. And in cities and states that specifically set out to test protestors, like Massachusetts, Seattle, and Minnesota, the results have shown that demonstrators were not considerably more likely to test positive compared to the general population. That’s not to say protesting is entirely without risk. “Mixing in large groups increases the probability of transmission. I don’t think that’s controversial,” says Chad Cotti, a professor of economics at University of Wisconsin-Oshkosh. But, he adds, “how much transmission you get is clearly going to be a function of the environment and the circumstances. Are people wearing masks? Are people physically touching each other? Is it indoors, is it outdoors?” We may yet see a protest-related spike in coronavirus cases. Many of the demonstrators were young, and thus likely to develop only mild symptoms from COVID-19, if any at all. But even asymptomatic or mildly symptomatic people can carry the virus to older, more vulnerable people in their homes or communities. If that’s happening, it would take more time to show up in the data. Still, the lack of notable protest-related spread so far offers valuable lessons for managing the ongoing pandemic. It’s further evidence, for instance, that being outside with other people is relatively safe. Furthermore, many of the protestors wore masks to protect themselves and the people around them, which experts say significantly reduces the risk of transmission. “What I’ve seen supports things that we already knew, which are that if you’re going to gather, being further apart is better than being stuck close together, that being is masked is better than being unmasked, and that being outside is better than being inside,” says Janet Baseman, a professor of epidemiology at the University of Washington. This isn’t to say that the disease didn’t spread at all during the protests. In Los Angeles and Washington, D.C., respectively, several police officers and members of the D.C. National Guard tested positive following the demonstrations; law enforcement groups nationwide have been criticized for failing to wear masks during the demonstrations. Furthermore, smaller protests have continued through June, and it will take time before any spread of the virus at these more recent events shows up in the data. While cases of COVID-19 have risen in some cities where major protests occurred (like Atlanta, Phoenix and Houston), experts say that’s likely not because of the demonstrations, but because of relaxed rules regarding indoor gatherings in those areas. “I think indoor transmission, events that might be happening at bars, are more important for the trajectory of the virus than the protests were,” says Dr. Amesh Adalja, an infectious disease and pandemic preparedness expert at the Johns Hopkins Center for Health Security. “What the protests added wasn’t as impactful as some of the other changes that were going on in society at the same time.” The George Floyd protests may have had a surprising effect that could have slowed COVID-19 transmission: In one study still undergoing peer review, researchers analyzing cell phone location data found that people in cities rocked by protests were more likely to stay home, perhaps due to curfews enacted amid the protests, or—especially in places where police violently cracked down on demonstrators—fear of getting caught up in the mayhem. “Even if there is an increase in the number of cases among the protesters themselves, to one extent, if the non-protesting population is engaging in greater social distancing, they are not going outside their house as much as they did…that counteracts any increase,” says Dhaval Dave, a professor of economics at Bentley University and a co-author of the study. So far, the lack of notable protest-related viral transmission would seem to justify the beliefs of the many doctors and other medical experts who expressed support for the protests, despite the immediate risk to public health. Moving forward, experts say, demonstrators should seek to keep following official guidance as much as possible. “I think wearing a mask, and social distancing, and being outside as much as possible, are the key things that we can do, that we know work,” says Roger Shapiro, associate professor of immunology and infectious diseases at Harvard’s School of Public Health. “And that’s what I hope protected most of the protesters.” from https://ift.tt/31vcRl7 Check out https://takiaisfobia.blogspot.com/
0 Comments
(WASHINGTON) — Dr. Anthony Fauci said coronavirus cases could grow to 100,000 a day in the U.S. if Americans don’t start following public health recommendations. The nation’s leading infectious disease expert made the remark at a Senate hearing on reopening schools and workplaces. Asked to forecast the outcome of recent surges in some states, Fauci said he can’t make an accurate prediction but believes it will be “very disturbing.” “We are now having 40-plus-thousand new cases a day. I would not be surprised if we go up to to 100,000 a day if this does not turn around, and so I am very concerned,” said Fauci, infectious disease chief at the National Institutes of Health. Fauci said areas seeing recent outbreaks are putting the entire nation at risk, including areas that have made progress in reducing COVID-19 cases. He cited recent video footage of people socializing in crowds, often without masks, and otherwise ignoring safety guidelines. from https://ift.tt/3ghIfYF Check out https://takiaisfobia.blogspot.com/ WASHINGTON — A leading Republican senator says President Donald Trump should start wearing a mask at least some of the time because politics is getting in the way of protecting the American people from COVID-19. “The stakes are too high for the political debate about pro-Trump, anti-Trump masks to continue,” says Sen. Lamar Alexander of Tennessee. Alexander is chairing a hearing of the Health, Education, Labor and Pensions committee that’s focused on ways to safely reopen schools and workplaces. Alexander had to self-quarantine after he was exposed to a staff member who tested positive. But the senator says he was protected because the staffer was wearing a mask. from https://ift.tt/2BfoZfB Check out https://takiaisfobia.blogspot.com/ Summer has just begun, but health officials are already warning Americans that the fall and winter months ahead will likely be challenging. Once flu season begins, the U.S. will have to worry about not one, but two contagious viruses. “The real risk is that we’re going to have two circulating respiratory pathogens at the same time,” said Dr. Robert Redfield, Director of Centers for Disease Control and Prevention (CDC) during a TIME 100 Talks discussion with senior health writer Alice Park. “We know flu by itself can cause substantial morbidity and mortality and hospital utilization,” especially for elderly people and those who have underlying health conditions. With the new coronavirus wreaking devastation in these groups and others, “this could be really a very, very difficult situation.” Getting a flu vaccine is one way to help prevent influenza. But even though flu vaccines are safe and often quite effective, they aren’t very popular. “Historically, less than half of Americans get flu vaccines,” Redfield said. “This is the year that I’m asking the American public to seriously reconsider, because that decision may make available a hospital bed for somebody else that really needs it for COVID.” So far this summer, as states have begun to reopen, Redfield said more than 100 counties in the U.S. are “what we consider [coronavirus] hot spots” and “experiencing higher transmission rates than we would like to see.” In response, he said, the CDC is sending teams to those areas and working with state and local health officials to understand how those cases are spreading and how best to contain them. Redfield also denied that the CDC has been sidelined during the pandemic; in previous outbreaks, the CDC has taken a more visible role in holding press conferences to educate and answer questions from the public. “I’d say no,” Redfield said in response to whether the agency has been taking a backseat in guiding the country through the pandemic. “We have a seat at the table in the {White House Coronavirus] Task Force where I represent the CDC…and we are presenting those view and I can tell you those views are heard, and those views are respected.” Right now, the tools Americans have been using for months—standing six feet apart, wearing face coverings, washing hands regularly—are still the best protections against contracting the virus that causes COVID-19. But by late 2020 or early 2021, that arsenal may realistically include one or more coronavirus vaccines, Redfield said. That’s an incredibly quick timeline for a vaccine of this kind, and three months ago, Redfield would have called it “highly optimistic.” Now, though, “I think there’s a real probability that we’re going to accomplish that. No one can guarantee it, but the amount of progress that’s been made in recent weeks is substantial.” This article is part of #TIME100Talks: Finding Hope, a special series featuring leaders across different fields encouraging action toward a better world. Want more? Sign up for access to more virtual events, including live conversations with influential newsmakers. from https://ift.tt/31u1ry0 Check out https://takiaisfobia.blogspot.com/ We Have a Cheap Effective Way to Keep Ourselves Safer From COVID-19. Why Are We Fighting About It?6/29/2020 At long last, we have made a truly game-changing scientific breakthrough in preventing the spread of COVID-19. The impact of this breakthrough seems almost too good to be true. We have found a disease control tool that, when used properly, can dramatically reduce the person-to-person transmission of SARS-CoV-2, the virus that causes COVID-19. Studies have shown that this tool could reduce transmission by somewhere between 50% and 85%. The tool is cheap and remarkably low-tech. You can even make one at home. It has no significant side effects. And with each passing day, the scientific research showing the tool’s effectiveness gets stronger and stronger. If this tool were a vaccine or medicine, we’d be high-fiving each other and popping the champagne, knowing we’d discovered a crucial means to help prevent the spread of the pandemic. I’m talking, of course, about face masks—cloth, surgical, or even a bandanna. Face masks block the spread of respiratory droplets that can carry the novel coronavirus. But just as with so many other aspects of the response to COVID-19—including mass testing, contact tracing, and the early use of stay-at-home orders—the U.S. is once again squandering this opportunity. In many countries that have so far successfully controlled their COVID-19 epidemics, public health leaders, politicians, and the public have fully embraced the use of face masks with no hint of controversy. A recent study found that countries where masks were widely used soon after their COVID-19 outbreak began were more likely to keep their death rates low and to have a shorter outbreak. Countries like Hong Kong, South Korea, Taiwan, Thailand, and Vietnam that quickly adopted masking, along with other control measures such as social distancing and track and trace, have reported fewer than 6 deaths per million residents as a result of COVID-19. Yet in the U.S., where the death rate from COVID-19 is now 379 per million people, face masks have been weaponized for partisan purposes. Taking their cues from President Trump, who has refused to appear on camera wearing a face mask and has said that Americans who wear masks are doing so to show their disapproval of him, many of his supporters now see wearing a face mask as an affront to personal liberty. According to the Washington Post, Republican leaders “are less likely to mandate them, and Republican voters are more likely to forgo, and even scorn, them.” Health officials who have promoted mask mandates have quit their jobs after receiving death threats. As a result of this alarming polarization, only 18 states and the District of Columbia are mandating face masks in public across the whole state. Only two—Massachusetts and Maryland—have Republican governors. Meanwhile, many Republican-led states are actively trying to subvert local measures. Nebraska Governor Pete Ricketts has gone so far as to say he will withhold federal coronavirus relief funds from local governments if they try and mandate mask use in their places of work. Rejecting face masks inevitably means embracing more COVID-19 cases and deaths. One U.S. study found that states with a mandate had a more rapid decline in daily growth rates of COVID-19 and estimated that mask use prevented up to 450,000 cases of COVID-19 by May 22, 2020. And while researchers at the University of Washington now predict that the U.S. could reach 180,000 COVID-19 deaths by October, they say we could prevent 33,000 of these deaths—more than half of the new deaths the model projects—if at least 95% of people wear a mask. That’s right. We can avert the deaths of 33,000 of our parents, grandparents, siblings, co-workers, teachers, bus drivers, mail carriers, nurses and store and factory workers by just sticking a one-dollar piece of cloth over our noses and mouths. So what’s stopping us? One problem is the “me first” culture in the U.S., in which anti-maskers claim that their right to go around unmasked in public matters more than saving lives. What they don’t seem to get is that while masks may protect the wearer, the more important reason for wearing them is to protect others. If you are infected but don’t know it—because you have no symptoms (“asymptomatic infection”) or the symptoms have not yet appeared (“pre-symptomatic infection”)—a mask reduces the risk that you will spread the virus to others around you. What’s more, the higher the proportion of people who wear masks, the lower the risk that the coronavirus will spread through the community, akin to herd immunity after vaccination. Once a certain percentage of people, known as a “herd,” is vaccinated (e.g. 95% in the case of measles vaccine), then the unvaccinated people also become protected. Similarly, mass masking provides benefits across a whole community. This is why it is so important for governments to issue and enforce mask mandates. Not surprisingly, the rate of mask use is much higher in states with mandates. The highest rates of mask use (60%-70%) are in the Northeast—Connecticut, Maine, Massachusetts, and Rhode Island, all of which have statewide mandates. The lowest rates (under 10%) are in Arizona, Indiana and Tennessee, none of which have state mandates. COVID-19 cases are on the rise in again 31 states—and growing exponentially in crisis states like Arizona, Texas, and Florida that acted much too quickly to reopen businesses. The only way to control the dramatic rise in these “humanitarian catastrophe” states will be to reinstate full lockdowns and mandatory social distancing. Mass masking isn’t the way to end a huge surge in COVID-19. Instead, it is one of the ways that we can help avoid repeated cycles of lockdown and release. There is plenty of evidence from countries around the world that widespread mask wearing—in combination with 2 meters of social distancing, handwashing, and track and trace testing—will allow us to more safely do the things we so desperately want and need to do: go back to work, reopen schools, see friends and family, and restart our economy. But to have any success, we need to reframe and depoliticize the wearing of face masks. I have been encouraged to see some Republicans—including Mitch McConnell, Marco Rubio, Arnold Schwarzenegger and even Dick Cheney—publicly endorse the importance of wearing masks. That support needs to gain steam in state legislatures and governor’s offices. Leaders further need to strongly and publicly condemn the fringe who are spreading misinformation about masks and openly flouting public health guidelines. Wearing a face mask is not is sign of weakness. It is an act of solidarity, an expression that all of us—Democrats, Republicans and Independents—have a role to play in defeating one of the greatest public health challenges we have faced in our lifetimes. from https://ift.tt/3eKCL8p Check out https://takiaisfobia.blogspot.com/ Liz Satterfield has a ritual for every time she returns home after leaving the house. Diagnosed with metastatic breast cancer in 2016, the Kirkland, Washington resident recently learned that the cancer that had spread to her brain in 2018 was still growing. Throughout the pandemic, she’s had to visit the hospital at least once every three weeks, often more frequently, for treatments to control her disease. “I have a pair of shoes in a paper bag that I keep in the trunk of my car or a rack in the garage. I only wear those shoes when I’m going in to get treatment,” she says. “When I come home, I strip in the garage and put everything right in the wash. I don’t enter the house with anything that I was wearing at the cancer center. It’s the way I’m able to control what I can control in this situation, and gave my partner and me some peace of mind.” While COVID-19 has upended everyone’s life, the novel coronavirus’ impact on cancer patients is especially disruptive. Any infectious disease that taxes the immune system is high on their must-avoid list—especially for those getting chemotherapy or radiation treatments, both of which can weaken natural defenses. So that leaves cancer patients caught in the middle of two terrifying diseases. Nearly 17 million people in the U.S. are living with cancer, many of whom, like Satterfield, are currently being treated for their disease, and forced to make these difficult calculations weighing their risk of cancer against their risk of getting COVID-19. Studies of cancer patients who become infected suggest that their death rate is higher—ranging from 13% to 28%—than those without cancer (though these numbers continue to change as more data become available). That risk could have a lasting impact on cancer rates and deaths in coming years. Between existing cancer patients who are concerned about the risk of COVID-19 and either delay or skip treatments, and those who have not yet been diagnosed but are reluctant to see their doctor for possible cancer symptoms, experts say both death rates and new cases may creep up. “There have been people who are scared to death to even come near the cancer center,” says Dr. Leslie Busby, a partner at Rocky Mountain Cancer Centers. A crude forecast of how the pandemic might affect deaths from just breast and colon cancers alone conducted by researchers at the National Cancer Institute (NCI) predicts 10,000 additional deaths from these two cancers on top of an expected 1 million over the next decade, based on the assumption that screenings are stopped for only six months. That model does not account for people who have not yet been diagnosed and are delaying seeing their doctors—and as a result, may not be diagnosed until their cancers are more advanced and harder to treat. “We don’t know what the level of disruption to care is going to be, but I think it has already been quite significant, and will last a while longer,” says Dr. Ned Sharpless, director of the NCI, who commissioned the prediction. He notes that increases in incidence and deaths from cancer due to COVID-19 may also be hidden, complicated by the fact that incidence, for example, may even dip for a while if fewer people are getting screening and fewer cancers are actually detected. Mortality may also be confounded by the fact that most cancer deaths are among older patients, and older patients are also at higher risk of dying from COVID-19 complications, so the pandemic could cause total cancer deaths to actually decrease tempoerarily. Given those confounders, and the fact that many cancers take years to develop, it won’t be clear exactly how COVID-19 has affected cancer rates and deaths for many years yet. “When you think of cancer care, there is very little that is elective,” says Dr. Robert Keenan, chief medical officer and vice president of quality at Moffitt Cancer Center in Tampa, Fl. Patients get chemotherapy as an intravenous infusion, which needs to be dosed and administered under medical care, and radiation treatments require calibrated doses from certified technicians in hospitals. And once patients have started chemotherapy or radiation regimens, they usually undergo treatment for several weeks, with each cycle building on the last to give them the best chance of wearing the cancer down and stopping malignant cells from growing and spreading. As the pandemic began to surge, cancer doctors typically evaluated each of their patients to decide whether they needed to come in for their treatments or whether they could safely put off the chemotherapy infusion or radiation session for a week or more. Nancy Fleming, a former hospital pharmacist who was diagnosed with small cell lung cancer in 2019 after surviving breast cancer in 2003, receives an infusion of an immunotherapy drug once a month at the Dana Farber Cancer Institute in Boston, Mass. When cases of COVID-19 surged in Boston in April, her oncologist, Dr. Jacob Sands, suggested she put off one of her infusions by a week. He says he made these types of decisions on a case-by-case basis, depending on how well each individual patient was doing and how well-controlled their cancer was. “For somebody who has ongoing disease control, where everything is stable, and they had been on therapy for more than a year, those were cases where we would discuss delaying treatment by a week, two weeks or even three weeks,” Sands says. Convincing them to continue their treatments wasn’t easy, however. “There was a lot of virtual and telephonic hand-holding,” says Keenan. “We tried to put in place measures to create an environment that let patients know that [the cancer center] was as safe a place as any to come in for their treatment.” At many hospitals and cancer centers, patients and staff have been screening patients and staff for fever and COVID-19 symptoms, and many restricted visitors from coming with the patients for their treatments. Any care that could be provided virtually was moved to video or telemedicine, which cut down on the density of people. At Moffitt, Keenan says, clinic visits dropped by 40% to 50%, and patient appointments were scheduled to avoid pile ups waiting rooms. At Dana Farber, Sands says “Patients were essentially able to get right into a private room when they showed up and we were able to completely isolate people so they were not sitting next to each other in the waiting room.” Such cues are critical to putting cancer patients’ at ease, agrees Busby, who asked non-essential staff to work from home. “These practices helped to both lower the risk of spreading COVID-19 and sent signals to our patients that we were doing the best we can to protect their health,” he says. Discussing these precautions helped to convince some wary patients to continue their treatments. One such policy, however, was harder for patients to accept. Many cancer centers stopped allowing visitors to come with patients during their treatment appointments, which can stretch for several hours since the chemotherapy infusions themselves typically take at least 30 minutes. “It’s such a comfort to have family there,” says Fleming. “When you are a patient, when you are ill, it’s sometimes hard for you to absorb everything you are hearing. It’s always good to have an advocate with you.” For breast cancer patients, there were other options as well. At the University of North Carolina Lineberger Comprehensive Cancer Center, Dr. Lisa Carey says the pandemic changed the therapies she offered her patients. At the beginning of the pandemic, “for the patients whose cancers were hormone sensitive, I put them on anti-estrogen [pills] so we could tread water and keep an eye on the tumor for a couple months, while we waited for the [COVID-19] dust to settle before exposing them to an unknown level of danger of coming into the hospital for chemotherapy infusions,” she says. The oral treatment, normally given before or with chemotherapy for maximum effectiveness, allowed the patients to treat their cancer and not compromise their care while avoiding exposure to the risks of COVID-19 in the hospital. “The truth is, those things we did to protect them seemed to work,” Carey says. Protecting patients from getting exposed to the virus also guides some of her decisions around how to provide chemotherapy. “If I have a choice between a [chemotherapy] drug that is given every week and a similar one that is given every three weeks, I now routinely use the one that’s given every three weeks,” she says. “Even if there are a few more side effects, if it reduces the number of times a patient has to come in, then this is a conversation I’m having with them.” Similar adjustments are possible for radiation treatment in some cases. Normally, radiation therapy is broken up into smaller, daily fractions in order to preserve the healthy tissue around cancers from the toxic effects of single blast. For breast cancer patients, recent, albeit early studies that followed patients for five years, suggested that significantly shorter courses of treatment—given over five days compared to 30, for example—could be equally as effective in controlling the cancer. “Typically we wouldn’t embrace [such early results] in daily practice as quickly as we did except for the pandemic,” says Dr. Reshma Jagsi, deputy chair of radiation oncology at the University of Michigan. “But some patients were willing to take the risk of not having long term evidence on the safety and trust the five year data which was certainly compelling and intriguing.” For the most part, cancer patients have understood the importance of continuing their treatment and of balancing their risk of cancer against their risk of getting COVID-19. In fact, says Busby, “it’s not so much our patients we worry about but the patients who are not ours yet.” Most hospitals canceled routine cancer screening appointments for things like mammograms and colonoscopies, which are essential for detecting cancer early. And many people who might have potential cancer symptoms and aren’t diagnosed yet, aren’t going to the doctor because of COVID-19 fears. If that’s the case—and only data on cancer rates in the coming months and years will provide the answer—it’s possible that both the number of new cancer cases and their severity will increase as a result of the pandemic. “My concern is for the patients who have not yet been diagnosed with cancer; for those patients who delayed their screening; for patients who put off being examined for certain symptoms,” says Jagsi. “Those patients will be diagnosed at later stages and I do have great concern there that will change cancer-related treatment outcomes.” In recent years, advances in screening have helped doctors more regularly diagnose patients at earlier stages where their disease is still treatable and curable, Jagsi notes. “I fear that some COVID-19-related delays may compromise some of the advances we have seen.” How deeply COVID-19 will cut into those gains won’t be clear until more data on new cancer cases becomes available in coming months. But most experts agree that “it’s hard to imagine that the pandemic would contribute to a better situation; it’s going to have to be worse,” says Carey. In the meantime, patients are learning to accept the adjustments they need to make to ensure their treatments continue with as little disruption and in the safest way possible. Satterfield has had two COVID-19 tests because the chemotherapy she receives gives her a runny nose, cough and diarrhea—all symptoms of COVID-19 that are flagged when she is screened before entering the cancer center for her treatments. But she’s okay with that, and understands why it’s needed. For her, “the most challenging part is emotional. With any terminal illness, it’s there—I think, is this the way the world is going to be when I die? Is this how I see the end of my life? But I’m feeling better than I have in recent memory. As much as my health status doesn’t sound great, I feel great. And I’m thankful for that.” from https://ift.tt/2BkoYa5 Check out https://takiaisfobia.blogspot.com/ The World Hits Sobering Coronavirus Milestones: 500000 Dead and 10 Million Confirmed Cases6/28/2020 (ROME) — The world surpassed two sobering coronavirus milestones Sunday — 500,000 confirmed deaths, 10 million confirmed cases — and hit another high mark for daily new infections as governments that attempted reopenings continued to backtrack and warn that worse news could be yet to come. “COVID-19 has taken a very swift and very dangerous turn in Texas over just the past few weeks,” said Gov. Greg Abbott, who allowed businesses to start reopening in early May but on Friday shut down bars and limited restaurant dining amid a spike in cases. California Gov. Gavin Newsom rolled back reopenings of bars in seven counties, including Los Angeles. He ordered them to close immediately and urged eight other counties to issue local health orders mandating the same. More Florida beaches will be closing again to avoid further spread of the new coronavirus as officials try to tamp down on large gatherings amid a spike in COVID-19 cases. Florida Gov. Ron DeSantis said interactions among young people are driving the surge. “Caution was thrown to the wind and so we are where we are,” DeSantis said. South Africa’s health minister warned that the country’s current surge of cases is expected to rapidly increase in the coming weeks and push hospitals to the limit. Health Minister Zwelini Mkhize said the current rise in infections has come from people who “moved back into the workplace. New clusters of cases at a Swiss nightclub and in the central English city of Leicester showed that the virus was still circulating widely in Europe, though not with the rapidly growing infection rate seen in parts of the U.S., Latin America and India. Poland and France, meanwhile, attempted a step toward normalcy as they held elections that had been delayed by the virus. Wearing mandatory masks, social distancing in lines and carrying their own pens to sign voting registers, French voters cast ballots in a second round of municipal elections. Poles also wore masks and used hand sanitizer, and some in virus-hit areas were told to mail in their ballots. “I didn’t go and vote the first time around because I am elderly and I got scared,” said Fanny Barouh as she voted in a Paris school. In Texas, Abbott appeared with Vice President Mike Pence, who cut campaign events from upcoming visits to Florida and Arizona because of rising virus cases in those states. Pence praised Abbott for both his decision to reopen the state, and to roll back the reopening plans. “You flattened the curve here in Texas … but about two weeks ago something changed,” Pence said. Pence urged people to wear masks when unable to practice social distancing. He and Abbott wore face masks as they entered and left the room, taking them off while speaking to reporters. Health and Human Services Secretary Alex Azar, meanwhile, defended the fact that President Donald Trump has rarely worn a mask in public, saying he doesn’t have to follow his own administration’s guidance because as a leader of the free world he’s tested regularly and is in “very different circumstances than the rest of us.” Addressing spikes in reported coronavirus cases in some states, Azar said on NBC’s “Meet the Press” that people “have to take ownership” of their own behaviors by social distancing and wearing masks if possible. A reported tally Sunday from Johns Hopkins University researchers said the death toll from the coronavirus pandemic had topped 500,00. About 1 in 4 of those deaths – more than 125,000 – have been reported in the U.S. The country with the next highest death toll is Brazil, with more than 57,000, or about 1 in 9. The true death toll from the virus, which first emerged in China late last year, is widely believed to be significantly higher. Experts say that especially early on, many victims died of COVID-19 without being tested for it. To date, more than 10 million confirmed cases have been reported globally. About a quarter of them have been reported in the U.S. The World Health Organization announced another daily record in the number of confirmed coronavirus cases across the world – topping over 189,000 in a single 24-hour period. The tally eclipses the previous record a week earlier at over 183,000 cases, showing case counts continue to progress worldwide. Overall the U.S. still has far and away the most total cases. At more than 2,450,000 – roughly twice that of Brazil. The number of actual cases worldwide is much higher. New York, once the nation’s pandemic epicenter, is now “on the exact opposite end,” Gov. Andrew Cuomo said in an interview with “Meet the Press.” The state reported five new virus deaths Saturday, its lowest reported daily death toll since March 15. During the state’s peak pandemic in April, nearly 800 people were dying every day. New York still leads the nation in COVID-19 deaths with nearly 25,000. In the state of Washington, Gov. Jay Inslee put a hold on plans to move counties to the fourth phase of his reopening plan as cases continue to increase. But in Hawaii, the city of Honolulu announced that campgrounds will reopen for the first time in three months with limited permits to ensure social distancing. Britain’s government, meanwhile, is considering whether a local lockdown is needed for the central English city of Leicester amid reports about a spike in COVID-19 among its Asian community. It would be Britain’s first local lockdown. “We have seen flare-ups across the country in recent weeks,” Home Secretary Priti Patel told the BBC on Sunday. Polish voters were casting ballots, in person and by mail, for a presidential election that was supposed to have taken place in May but was chaotically postponed amid the pandemic. President Andrzej Duda, a 48-year-old conservative backed by the nationalist ruling Law and Justice party, is running against 10 other candidates as he seeks a second five-year term. Iwona Goge, 79, was encouraged to see so many people voting in Warsaw. “It’s bad. Poland is terribly divided and people are getting discouraged,” she said. French voters were choosing mayors and municipal councilors in Paris and 5,000 towns and cities in a second round of municipal elections held under strict hygiene rules. Key battlegrounds include Paris, where the next mayor will preside over the 2024 Summer Olympics. Italy was honoring its dead later Sunday with an evening Requiem concert in hard-hit Bergamo province. The ceremony in the onetime epicenter of the European outbreak came a day after Italy registered the lowest daily tally of COVID-19 deaths in nearly four months: eight. European leaders were taking no chances in tamping down new clusters. German authorities renewed a lockdown in a western region of about 500,000 people after about 1,300 slaughterhouse workers tested positive. Africa’s confirmed cases of COVID-19 continued to climb to a new high of more than 371,000, including 9,484 deaths, according to figures released Sunday by the African Centers for Disease Control and Prevention. ___ Associated Press journalists around the world contributed to this report. from https://ift.tt/2NJ42vP Check out https://takiaisfobia.blogspot.com/ (CARROLLTON, Texas) — A surprise birthday party that resulted in 18 people testing positive for the coronavirus has left a North Texas man horrified as his father continues to fight for his life in a hospital intensive care unit. Ron Barbosa, who is married to a doctor and refused to attend the May 30 party for his daughter-in-law because of safety concerns amid the COVID-19 pandemic, said those hospitalized included his parents, both in their 80′s, and his sister, who is also battling breast cancer. Barbosa said his nephew, unknowingly infected with the virus, hosted last month’s gathering of 25 people that only lasted a few hours. During the party, he said the nephew interacted with seven relatives, who subsequently contracted the virus and spread it to 10 other family members, including two young children. Read more: America Is Done With COVID-19. COVID-19 Isn’t Done With America “When people started getting sick, we really let everyone have it,” Barbosa told WFAA-TV. “We knew this was going to happen, I mean, this whole time this has been going on we’ve been terrified.” Gov. Greg Abbott on Thursday said Texas would halt its aggressive reopening as it deals with a surge in coronavirus cases and hospitalizations that has made the state a virus hot spot. Statewide, the number of COVID-19 patients has more than doubled in two weeks. Texas has reported more than 11,000 new cases in the previous two days alone. Barbosa’s mother, Carole, who stopped by the function to drop something off, tested positive for coronavrius June 6 and was admitted to the hospital a week later. Barbosa said his father, Frank, who didn’t attend the get-together but later contracted COVID-19, was hospitalized June 17. He said his dad is currently “hanging on by a thread” in the ICU while on life support. “It’s heartbreaking,” Barbosa said, holding back tears. Frank received a plasma donation Wednesday from a recovered coronavirus patient, according to Barbosa’s Facebook page. Barbosa said he hopes the procedure will save his dad’s life. “Prayers were answered today,” Barbosa wrote on Facebook. “Now he (Frank) needs to get well for mom and the Barbosa Family.” Barbosa said his family remains united despite feeling a pendulum of emotions over the past few weeks. “We were horrified. People couldn’t believe that they took it to a family member,” he said. “But now, we’re holding on together.” Carole has returned home to recover, according to a Facebook page the family created, which indicated that Barbosa’s sister, Kathy, is feeling better and back home to recuperate. from https://ift.tt/31ldm1h Check out https://takiaisfobia.blogspot.com/ A large European study confirms a rare bit of good news about COVID-19: children seem to be mostly spared from the worst of its effects. The paper, published June 25 in the Lancet Child & Adolescent Health, suggests well fewer than 1% of children who develop COVID-19 will go on to die from it, and the vast majority will not need intensive care. By contrast, in some of the world’s hardest-hit countries, case fatality ratios that include adults are estimated (albeit using preliminary data) to be higher than 10%. The new study analyzed case data from almost 600 pediatric COVID-19 patients from 21 different European countries. The kids ranged in age from three days to 18 years old, and boys made up just over half of the group. Three-quarters of the children had no preexisting medical conditions. More than half of the children were admitted to a hospital, but only 8% required intensive care, the researchers found. Only four patients died from their disease. That works out to a case fatality rate of 0.69%. Across entire populations, the actual rate is probably much lower, the researchers write, since many children infected with COVID-19 have such mild cases they never require medical care in the first place, let alone need to be admitted to a hospital. For example, 16% of kids in the study never showed COVID-19 symptoms; many of them were only tested because they’d had close contact with another infected person. The researchers found that infants younger than one month of age were more likely than older children to need intensive care—but, interestingly, all four of the patients who died were older than 10. Two of the children who died had pre-existing medical conditions, a known risk factor for more severe disease. As with adults, boys were more likely to be require intensive care than girls, according to the study. “Co-infection” with another virus—like influenza or another strain of coronavirus—also seemed to increase the severity of a child’s disease, which the researchers write “might have implications for the winter period 2020–21, when the incidence of other viral respiratory tract infections…is bound to increase.” The study’s data were gathered from April 1 to April 24, before a string of reports suggested a possible connection between COVID-19 and a pediatric inflammatory condition similar to Kawasaki disease. That condition, which can lead to shock and fatal heart damage, remains very rare, and researchers are still determining exactly how, if at all, it relates to coronavirus. The new paper comes as the median age of COVID-19 patients is trending downward in the U.S. The shift in demographics seems to be driven mostly by younger adults—not children—getting infected in larger numbers, as well as better testing protocols. Research in the U.S. and abroad still suggests kids are far less likely than adults to develop a serious case of coronavirus. from https://ift.tt/2VlV63M Check out https://takiaisfobia.blogspot.com/ The U.S. Has Officially Unflattened the Curve With Its Worst Day of the Coronavirus Pandemic Yet6/25/2020 On April 7, less than a month after reported cases of COVID-19 began to rise in the United States, the rate of new infections reached a peak: an average of 31,630 new cases per day, meaning close to 10 in every 100,000 Americans were testing positive daily. For months, that figure stood as the worst day in the pandemic’s spread at the national level. Until now. The latest data show that, on Tuesday and Wednesday of this week (June 23 and June 24), the U.S. surpassed that high-water mark, at more than 31,700 infections per day. The state of the pandemic in this country is officially worse than it has ever been.  What is particularly troubling about this trend is that the country as a whole was on the right track through the end of May (unlike a number of states, such as North Carolina, which never flattened or showed extended signs of progress) even if it wasn’t out of the woods entirely. The fact that those positive signs all flipped in polarity suggest that, whatever combination of factors led to this resurgence, one thing is clear: the nation did not adapt to changing circumstances. Assigning causes and effects to peaks and valleys in a dataset as complex as this one is a dangerous business. But as my colleague Tara Law and I reported last week, greater availability of testing is very unlikely to explain the surge in cases. And one cannot ignore the fact that many states began cautiously reopening public spaces around Memorial Day, about two weeks before the numbers in the U.S. took off. That’s about COVID-19’s typical incubation time. The virus has also struck the country asymmetrically, moving from dense urban centers to less populated regions, which requires a nimble shift in public interventions to combat. Crunching the NumbersOne might reasonably ask why we didn’t notice this yesterday, since the peak value came two days ago. The answer involves just a smidgeon of math. We’ll get through it together. Every evening, a team at Johns Hopkins University publishes daily figures on the number of COVID-19 cases (and resultant fatalities) on a worldwide, national, U.S. state and U.S. county level. As you can see from the gray bars in the above chart, these figures, when graphed day-by-day (as opposed to cumulatively), can fluctuate a lot, for apparently arbitrary reasons. Figures tend to be higher on Fridays than earlier in the week, for example, which can easily make the trend hard to read on any given day if you don’t have weeks of data to help put it in context. What most publications (including TIME) have done is report the data in a seven-day rolling average, which smooths the curve in order to essentially imbue the chart with that context. We’re using what’s called a “centered” moving average, where each daily value shows the average of that day as well as the previous three days and the following three days. There’s one significant downside to this approach: the most recent few days don’t have seven data points to sample from, because, like you, we can’t see into the future. For those days, this method uses an average of the previous three days, the current day, and however many days follow (two, one, or none). But that’s a worthy trade-off for the fact that a centered average tracks much more closely with the raw data, showing a more accurate picture overall. That much is made clear from this comparison of the same data as above with an average of the previous week (blue), an average of the following week (green), and the centered average that TIME uses (red): 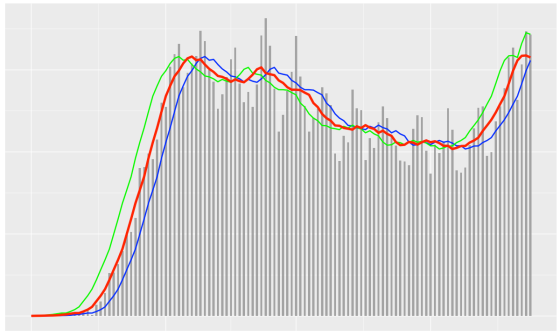
This may seem pedantic, but it gets to the heart of how tricky it can be to accurately report the magnitude of the COVID-19 crisis. Based on only the unaveraged daily values, the two worst days still lie in April, and that may be true for some time. And while as of today the centered average peaks on June 23, when we checked yesterday, with one fewer data point, June 23 was still a shade below the previous peak. Within a few days, we’ll be able to say for certain how much worse off we are now than we were when things previously looked the most bleak. from https://ift.tt/381RA3E Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
