|
As the school year gets underway and the Delta variant continues its march through the U.S. population, many parents with kids younger than 12 have the same question: When will vaccines become available for my child? No one knows exactly when the U.S. Food and Drug Administration (FDA) may grant one or multiple COVID-19 vaccines emergency-use authorization for children younger than 12. But Dr. Robert Frenck, director of the Vaccine Research Center at Cincinnati Children’s Hospital Medical Center and one of the investigators involved in testing Pfizer-BioNTech’s shot in kids, guesses parents will have to wait at least until October. On Aug. 24, National Institutes of Health Director Dr. Francis Collins said pediatric shots may not be approved before the end of 2021. That may seem ploddingly slow, given that Pfizer-BioNTech’s shot was authorized for 12- to 15-year-olds back in May. (Moderna submitted its shot for authorization among adolescents and teenagers in June, but the FDA hasn’t issued a decision yet.) But the research process is different for young children, who “are not just little adults,” says Dr. William Towner, physician director of clinical trials for the Kaiser Permanente Department of Research & Evaluation in Southern California. One major difference: 12- to 15-year-olds received the same vaccine dose as adults, whereas researchers have had to figure out the right amount to give to younger children. With smaller bodies—and immune systems that seem better prepared to fight off COVID-19—young kids should be able to get strong protection from a smaller dose, hopefully with fewer side effects, Frenck explains. After landing on the right doses for kids, trial sites moved into safety and efficacy testing, starting with children ages 5 to 11 and then moving down to toddlers and babies. That process is ongoing, and it was disrupted when the FDA in late July asked researchers testing both the Pfizer-BioNTech and Moderna vaccines to enroll additional children in their trials, in hopes of learning more about whether rare side effects, like heart conditions seen in a small number of teenagers after vaccination, also affect younger kids. Both Pfizer and Moderna are still recruiting participants for at least some of their study sites, but reaching that higher enrollment cap shouldn’t be a problem, Towner says. Kaiser Southern California is one of the sites across the country testing Moderna’s vaccine in kids younger than 12—and for each trial spot that opens up, Towner says he receives at least 10 applications from eager parents. “There’s definitely a strong interest in this clinical trial,” Towner says. “We’ve been getting a rather breathtaking response.” Even still, authorization for 5- to 11-year-olds is likely at least a few months off, Frenck guesses. Before granting emergency-use authorizations for adult and teen vaccines, the FDA reviewed two months of follow-up safety data from trial participants. It’s likely to want at least that much data from pediatric trials, and perhaps more. An FDA spokesperson referred TIME to agency documents and officials’ previous comments suggesting it will review at least two months of data for kids. A Pfizer spokesperson said in a statement to TIME that the company expects to have enough data to potentially support an emergency-use authorization for 5- to 11-year-olds by the end of September. Moderna representatives did not provide a statement before press time. Dr. Kari Simonsen, who is leading Omaha Children’s Hospital and Medical Center’s pediatric trial of the Pfizer-BioNTech vaccine, says she feels two months of follow-up is enough. “As a pediatrician, I do feel like using that same rationale that we did for adolescents and adults makes good sense,” Simonsen says. Her Nebraska hospital has already enrolled and vaccinated its 50 pediatric study participants and is now waiting for the FDA’s signal to move ahead. “It’s outside my hands,” Simonsen says. “I’m just anxiously awaiting when the FDA will take that up.” Many parents can’t wait for that day, as evidenced by the overwhelming response research centers around the country have gotten to their recruitment requests. That anticipation was seemingly only heightened when Pfizer-BioNTech’s shot received full FDA approval in August. In fact, after that approval, the American Academy of Pediatrics (AAP) issued a statement urging pediatricians not to prescribe the Pfizer shot off-label for children, apparently anticipating the wishes of concerned parents. “We do not want individual physicians to be calculating doses and dosing schedules one-by-one for younger children based on the experience with the vaccine in older patients,” Dr. Yvonne Maldonado, chair of the AAP committee on infectious diseases, said in the statement. “We should do this based on all of the evidence for each age group, and for that we need the trials to be completed. I know parents are anxious to protect their children, but we want to make sure children have the full benefit of ongoing clinical trials.” Even as some parents count down the days until pediatric shots are available, however, an even larger group remains skeptical. An international study published in November 2020 found that just 18% of parents said they would enroll their child in a vaccine trial. And in an August 2021 Kaiser Family Foundation survey, only 26% of U.S. parents with kids ages 5 to 11 said they would vaccinate them right away. Forty percent said they would “wait and see,” while 9% said they would vaccinate their kids only if required and 25% said they wouldn’t under any circumstances. Dr. Kelly Moore, president and CEO of the pro-vaccine Immunization Action Coalition, says pediatricians should start counseling parents about the benefits of vaccination as soon as possible, even though shots aren’t authorized for young kids yet. “Families are used to looking to their pediatrician for guidance on what happens to their child,” Moore says. “More than ever, the pediatrician’s ability to educate families is going to be critical.” Schools can play a similar role, particularly for kids who may not have regular interactions with a health care provider, she says. Frenck also urges parents to pay attention to current pediatric COVID-19 surges in parts of the South and Midwest, and to use that when making decisions about vaccination and other precautions. “We can show you that kids are getting sick, we can show you that kids are getting hospitalized, we can show you that kids are dying,” he says. “Please use that data.” from https://ift.tt/3kwDo9E Check out https://takiaisfobia.blogspot.com/
0 Comments
It’s clear that the Delta variant is more contagious than previous COVID-19 strains, as evidenced by the soaring case counts in the U.S. and around the world. But the big question has been whether it causes more severe disease than earlier versions of the virus that causes COVID-19. A peer-reviewed study published Friday in The Lancet Infectious Diseases suggests it can. According to the paper, people in England who got infected with the Delta variant were more likely to be hospitalized than those who got infected with the Alpha variant. The vast majority of the more than 43,000 COVID-positive people in the study were either unvaccinated or partially vaccinated. Relatively few of those 43,000 individuals—about one in 50, overall—were admitted to the hospital within two weeks of their first positive test, but infection with the Delta variant seemed to roughly double their chances after accounting for age and other risk factors. That finding tracks with previous research completed in Scotland and published in The Lancet in June. Infection with the Delta variant also raised someone’s chances of seeking emergency care, even if they were not ultimately admitted to the hospital, according to the new study. A little more than 4% of people who tested positive for the Alpha variant were admitted to the hospital or sought care in the emergency department within two weeks of their first positive test, compared to almost 6% of those infected by the Delta strain. The study analyzed U.K. hospital data from late March through late May 2021. In March, infections from the Alpha variant, which first emerged in the U.K. last year, outnumbered Delta cases. During the weeks at the end of the study period, the opposite was true. The study had a few limitations. The authors didn’t have access to data on underlying conditions, which are a known risk factor for more severe cases of COVID-19; they did, however, analyze patients’ ages, genders, ethnicities, socioeconomic statuses and travel histories. It’s also hard to control for personal factors that might make someone more or less likely to seek health care, such as individual risk tolerance or cultural norms. And, though the researchers tried to analyze only people who came to the hospital because of COVID-19, it’s possible that a small number of individuals were admitted for another reason and happened to test positive during routine screening. Finally, less than 2% of people in the study were fully vaccinated—a sample size too small to assess whether Delta also raises hospitalization risk among vaccinated people, the researchers wrote. If anything, that underscores the benefits of vaccination: so few immunized people tested positive for the virus, they barely showed up in the study population. Already in the U.S., Delta seems to be changing some people’s views of the pandemic. It has led to sobering spikes in pediatric hospitalizations—a wakeup call for many parents—and prompted some lawmakers to reimplement indoor mask mandates. It also seems to be inspiring people to get vaccinated in areas where it is spreading most. By illustrating how risky Delta can be to unvaccinated populations, the new research may keep that momentum going. from https://ift.tt/3zoVz7B Check out https://takiaisfobia.blogspot.com/ As the fourth wave of the COVID-19 pandemic continues, more companies are starting to require coronavirus vaccines for their employees. But this week, Delta Air Lines chose a different tactic when it became the first major U.S. company to say it will charge more for health insurance if employees do not get vaccinated. Some may see this as a compromise between vaccine mandates and more positive incentives, but experts say it could be complicated to execute and that there’s no way to tell how effective it will be. The move represents the tricky calculus employers are being forced to make as they try to keep employees safe and their companies running while avoiding the worker shortages hitting some industries. It also comes as vaccinated individuals around the country are blaming unvaccinated people for surging daily case numbers, resulting in increased hospitalizations, deaths, a return to mask-wearing and social-distancing measures, among other consequences. “We’ve always known that vaccinations are the most effective tool to keep our people safe and healthy in the face of this global health crisis,” Delta CEO Ed Bastian wrote in a memo to staff on Wednesday. “That’s why we’re taking additional, robust actions to increase our vaccination rate.” Starting on Nov. 1, Delta employees who have not been vaccinated will have to pay an extra $200 per month if they remain on the company’s health insurance plan. Delta justified the decision with the steep cost to the company of covering employees who are hospitalized due to the virus. Every Delta employee who has been hospitalized with COVID-19 was not fully vaccinated, the company said, and these hospitalizations cost an average of $50,000. Some experts say this doesn’t come as a surprise. A recent analysis from the nonpartisan Kaiser Family Foundation found that COVID-19 hospitalizations involving unvaccinated patients in June and July cost the U.S. health system a total of $2.3 billion. Hospitalizations have increased this month, which means the cost is likely to continue rising. “The cost impact is definitely a factor in employers and plans trying to encourage more people to get vaccinated through various mechanisms,” says Krutika Amin, associate director of KFF’s program on the Affordable Care Act and co-author of the analysis. Many parts of the corporate world have been considering—and implementing—various methods for getting people vaccinated in recent weeks. The National Football League said in July that teams with COVID-19 outbreaks among unvaccinated players will have to forfeit any games that can’t be rescheduled during the conference’s regular season. Major employers including Disney, Google, Walmart and Goldman Sachs have said they will require staffers to be vaccinated before returning to their offices. Some colleges and universities are charging unvaccinated students for regular coronavirus testing. And now that the FDA has fully approved the Pfizer vaccine, the Biden Administration has said all nursing homes that receive federal funding must mandate vaccines for their workers. Generally, employers can legally require that their employees be vaccinated as long as they provide accommodations for those who cannot get a vaccine due to a disability or sincerely held religious beliefs. About 14% of U.S. employers now require or plan to require their staff returning to worksites to be vaccinated, according to a recent survey from Mercer, a corporate benefits consulting firm. This is a significant increase from the 3% of employers who were doing so in a May survey. But Bastian, Delta’s CEO, told CNN this week he didn’t think a vaccine mandate fit with his company’s culture. At this point, 75% of the company’s staff is vaccinated, he said, and more than 80% of its pilots and flight attendants are vaccinated. “Every company has to make its own decision for its culture, its people, what works according to its values,” he said. “I think these added voluntary steps, short of mandating a vaccine, are going to get us as close to 100% as we can.” Delta employees who do not get vaccinated will also face other restrictions. They must immediately start wearing masks in all indoor settings, and they will have to undergo weekly COVID-19 testing starting Sept. 12. By the end of September, unvaccinated employees will stop receiving pay protection if they have to miss work due to testing positive for the virus. The insurance charge is more complicated than a straight mandate. Under federal law, insurers and employers cannot charge people more for pre-existing health conditions. But an exception in the Health Insurance Portability and Accountability Act (HIPAA) allows employers to use incentives as part of a workplace wellness program, and that’s how the coronavirus vaccine charges will be set up. However, some health care experts note that these kinds of premium incentives do not always work. The Affordable Care Act allows insurers to charge people more for smoking tobacco, and research has shown that tobacco-related surcharges do not lead people to stop smoking but do lead them to give up insurance coverage. Other studies have also shown little evidence for weight loss incentives and for workplace wellness programs more broadly. “I am very sympathetic to the complaints that those of us who are vaccinated can’t get back to our normal lives because of this group of people who are unvaccinated, and they’re going to cost the health system all this money,” says Sabrina Corlette, co-director of the Georgetown University McCourt School of Public Policy’s Center on Health Insurance Reforms. “But when the incentive is tied to the premium that somebody pays for their health insurance coverage, there’s no evidence that that particular incentive works.” The insurance charges are also likely to have the biggest impact on low-income people who may already be struggling to afford their health insurance premiums, Corlette says. Not having health insurance often deters Americans from seeking health care, and this could pose further problems at a time when politicians and public health officials are urging people to consult their own primary care doctors if they have questions about the vaccines. “Do we really want to price people out of insurance coverage that would give them access to a primary care provider who might be somebody that they trust and will listen to, and will help them understand the benefits of getting vaccinated?” Corlette asks. But Scott Ratzan, an expert in health communication at the City University of New York Graduate School of Public Health & Health Policy, says that while physicians are among the most trusted sources of information, he believes the added cost of an insurance surcharge might “wake up” people who have so far avoided getting vaccinated. “I think it’s a good thing that we start to remind people there’s a consequence for, frankly, bad decisions when it comes to not getting vaccinated. And these don’t only have consequences on themselves, they have consequences on all of society,” Ratzan says. He serves as executive director of Business Partners to CONVINCE, a global group of employers encouraging COVID-19 vaccination, and says he expects more companies to take similar steps soon. In some cases, firms may decide to implement extra insurance charges for unvaccinated employees if they believe their employees’ unions will not accept a vaccine mandate. For example, the Air Line Pilots Association’s Delta Master Executive Council, which represents 14,000 pilots at Delta, has already expressed concern about the company’s new policy. “The Delta MEC has consistently advocated to maintain the right of each individual pilot to consult with his or her medical provider regarding COVID-19 vaccinations or booster doses,” the union said in a statement. “While the Delta MEC respects Delta Air Line’s efforts to mitigate the impact of breakthrough COVID-19 variant infections, it needs to bargain with the Delta MEC over any employer-mandated vaccination for pilots.” And while such insurance charges are legal, some see the move as a slippery slope. Corlette would prefer companies mandate vaccination over tying the decision to health costs. “This is something that we fought long and hard about with the Affordable Care Act. Your health status or whether or not you sit on the couch all day and watch Netflix or jog every day—that shouldn’t be a factor in what a health insurance company can charge you as a premium,” she says. “It goes back to this kind of very fundamental question of, is access to health care a fundamental right, or is it a privilege?” from https://ift.tt/3BnqAtb Check out https://takiaisfobia.blogspot.com/ In the largest long-term study of COVID-19 patients yet to be published, researchers in China report in the Lancet worrying results of the disease’s lingering impact on people’s health. The scientists, led by Dr. Bin Cao from the China-Japan Friendship Hospital in Beijing, studied 1,276 people discharged between January to May 2020 from Jin Yin-Tan Hospital in Wuhan after being hospitalized for COVID-19. The patients all agreed to health visits at six and 12 months after their symptoms first appeared; at each of those points, the researchers compared the health status of the study participants with that of comparable people from the Wuhan area who did not experience COVID-19 infection. Among those hospitalized for COVID-19, 68% reported at least one continued, COVID-19-related symptom six months after their first symptoms appeared. While this percentage decreased by the 12-month mark, it remained relatively high, at 49%. And overall, patients who had been hospitalized for COVID-19 self-reported being in poorer health and having lower quality of life—including mobility issues— compared to controls. The most common symptom patients reported 12 months later was fatigue or muscle weakness; other issues included sleep disturbances, changes in taste and smell, dizziness, headache and shortness of breath. Certain symptoms were actually worse at the 12-month mark than they were earlier on in the study: the proportion of patients reporting breathing problems increased slightly, from 26% to 30%, from six months to a year following their first symptoms. The patients also filled out questionnaires about their mental health, and while 23% reported feeling anxious or depressed six months after their first symptoms appeared, 30% did so at a year. The findings highlight the complicated nature of COVID-19’s effects on people’s health, and the range of longer-term consequences emerging in what some experts are referring to as Long COVID. This recent study is the largest to date of such extended effects among hospitalized patients; while it suggests that about half of patients with serious COVID-19 recover from their symptoms, the other half—and especially those who were sicker during their hospitalization—may continue to battle the mental and physical effects of the virus for over a year. “I would not say this is a glass-half-full story,” says David Putrino, director of rehabilitation innovation at Mount Sinai Health Systems who oversees the network’s Long COVID rehabilitation program. “After most hospital stays, including for, say, walking pneumonia, I would not be expecting people at 12 months to still be reporting symptoms to me.” The increase in the proportion of patients experiencing anxiety or depression is especially “worrying,” say the authors, and they speculate that in addition to the isolation, unemployment, and loss of physical health that could be fueling these conditions, the virus itself may be driving abnormal immune responses that could affect the delicate work of brain chemicals contributing to people’s mental states. “Taken together, the implications are that people with persistent COVID-19 symptoms are looking at a long recovery,” says Putrino. At Mount Sinai’s Long COVID program that involves a personalized approach to addressing patients’ diverse symptoms, which could range from kidney, heart and lung problems to generalized fatigue and muscle weakness. For the latter, rehabilitation might include a tedious process of gradually stimulating the autonomic nervous system with carefully supervised exercises to slowly stimulate normal nerve activation, which could take as long as three to four months before patients feel better. “This virus doesn’t end once you get discharged from the hospital or once you get over the initial acute symptoms,” says Putrino. “This virus persists.” He notes that while the recent Lancet study only focused on hospitalized COVID-19 patients, other, albeit smaller, studies have shown that COVID-19 symptoms may linger in around 20% of those who get infected but don’t get sick enough to go to the hospital. That means the issue of persistent COVID-19 symptoms looms over any post-COVID-19 public health plan; currently, there isn’t much clarity about whether, or how much, insurers will cover rehabilitation for these patients. And that’s if patients know of and can access these services to begin with. “It’s the tip of the iceberg of enormous potential inequity and disparities in health,” says Putrino. “Most persistent symptoms are invisible symptoms, and walking into a doctor’s office and saying you have extreme fatigue”—a symptom many COVID-19 sufferers have reported experiencing months after infection—”[only] gets treated seriously when you’re not a member of a historically excluded group. And when you are, in many cases you don’t bother to even go to the doctor’s office because who is going to believe you?” from https://ift.tt/3ykuT6x Check out https://takiaisfobia.blogspot.com/ Aug. 20 was a good day in the pediatric intensive care unit at Children’s Hospital New Orleans. Carvase Perrilloux, a two-month-old baby who’d come in about a week earlier with respiratory syncytial virus and COVID-19, was finally ready to breathe without the ventilator keeping his tiny body alive. “You did it!” nurses in PPE cooed as they removed the tube from his airway and he took his first solo gasp, bare toes kicking. Downstairs, Quintetta Edwards was preparing for her 17-year-old son, Nelson Alexis III, to be discharged after spending more than two weeks in the hospital with COVID-19—first in the ICU, then stabilizing on an acute-care floor. “Fortunately, he never regressed,” Edwards says from outside Nelson’s room, the door marked with signs warning of potential COVID-19 exposure inside. “He’s progressing, slowly but surely.” The nurses and doctors who care for the sickest patients at Children’s Hospital New Orleans (CHNO) have to take the good where they can these days. On Aug. 6, Louisiana Governor John Bel Edwards announced that more than 3,000 children statewide had been diagnosed with COVID-19 over the course of just four days. That same week, about a quarter of Louisiana children tested for COVID-19 by the state’s largest health system turned out to have the virus. 
Seventy young patients ended up in treatment at CHNO during the 30 days ending Aug. 23. Prior to this summer, the hospital had never had to care for more than seven COVID-19 patients at a time, and usually fewer than that; on any given day in August, that number has been at least in the mid-teens, enough that the facility had to call in a medical strike team from Rhode Island to help manage the surge. CHNO isn’t alone. The extra-transmissible Delta variant has ushered in a new chapter of the pandemic. For the first time, pediatric hospitals are struggling to treat the number of young patients developing severe cases of COVID-19. A record high of more than 1,900 children were hospitalized nationwide on Aug. 14—and unlike during previous spikes, infections have so far been clustered largely in states with low vaccine coverage, meaning hospitals in undervaccinated states like Louisiana, Florida, Tennessee, Alabama and Texas are drowning. “Our hospital system across Alabama is beyond capacity. Last week we had net negative ICU beds, and that’s pediatric and adult together,” says Dr. David Kimberlin, co-director of the division of pediatric infectious diseases at Children’s of Alabama. “Doctors are doing CPR in the back of pickup trucks.” https://datawrapper.dwcdn.net/ZumvZ/2/ This grim scenario may seem shocking, given one of the pandemic’s long-standing silver linings: that children, for the most part, are spared from the worst of COVID-19. About 400 children nationwide have died from COVID-19 since the pandemic began, and most pediatric hospitals have seen no more than a handful of patients at a time—which makes the current surge in the South and parts of the Midwest especially unnerving. There is no evidence that the Delta variant is causing more severe disease than previous strains, says Dr. Sean O’Leary, vice chair of the American Academy of Pediatrics (AAP) committee on infectious diseases. Less than 2% of children who have caught COVID-19 during this wave landed in the hospital—roughly the same percentage as during earlier phases of the pandemic, according to a TIME analysis of AAP and U.S. Department of Health and Human Services data. An even smaller percentage of children die from the disease, though some have gone on to develop complications like the inflammatory condition MIS-C. 
The difference seems to be that the highly contagious Delta strain is tearing through all demographic groups at a furious clip, currently contributing to the more than 140,000 infections reported in the U.S. on any given day. It’s a depressing numbers game: If 100 children become infected, one or two might end up in the hospital. Push the caseload up to 180,000—the number of kids diagnosed with the virus nationwide during the week ending Aug. 19—and at least 1,800 are likely to get sick enough to need hospitalization. Children have also drawn a short straw. Viruses are wily, seeking out and infecting vulnerable hosts at all costs. Without authorized vaccines for people younger than 12, any child who has not previously been infected has no immunity against SARS-CoV-2, meaning the virus effectively has free rein among America’s 50 million youngest residents. Even among older children who can get vaccinated, rates are low: just 35% of 12- to 15-year-olds and 45% of 16- and 17-year-olds are fully vaccinated, according to U.S. Centers for Disease Control and Prevention data. While each individual child has a low chance of developing severe disease, the current pediatric surge, which has been compounded by an off-season spike in RSV and parainfluenza cases, has grave implications for health care networks. Even before the pandemic, health care access was a struggle in parts of the South and Midwest. In Arkansas, for example, there is only one pediatric hospital system to serve the state’s more than 3 million residents. A rural hospital could have fewer than 10 ICU beds, meaning even a small coronavirus surge could push it beyond its limits. “Down here in the deep South, we are getting slammed to the point where, honestly, our health systems may collapse,” Kimberlin says. “What that means is, if you have a stroke, you die at home.” There’s a reason pediatric ICUs are dangerously full in Tennessee and Texas but, at least at the moment, not Maryland and Massachusetts. In each of the latter two states, more than 60% of residents are fully vaccinated; in the former, about 41% and 46%, respectively. States with high vaccination rates also tend to be more aggressive about other precautions, like indoor mask mandates. https://datawrapper.dwcdn.net/n60o2/3/ There are exceptions—pediatric hospitalizations are ticking up in California (151 admissions this week vs. 68 a month ago) and New York (46 vs. 20 a month ago), two states with high vaccine coverage—and no one can predict what the virus will do in the future. But it stands to reason that more kids are getting sick in states like Louisiana, where only about 40% of the population is fully vaccinated and more than 4,600 new diagnoses are being reported among its 4.6 million residents each day. “Kids don’t tend to drive what’s going on; they tend to reflect what’s going on in the surrounding community,” O’Leary says. That children are largely at the mercy of the adults in their communities is one of the cruelest quirks of this surge. “It’s hard, because you don’t want to be judgmental” of people who haven’t gotten the shot, says Dr. Michael Blancaneaux, an emergency medicine physician at CHNO. 
But it’s also clear, he says, that the decisions of unvaccinated adults are endangering the lives of children who couldn’t be vaccinated even if they wanted to be. While many CHNO staff members are careful to say vaccination is a personal choice, there’s a discernible subtext beneath their politeness: they wish more people in the community would choose to vaccinate themselves and their families. For the doctors who treat young patients—and who are exhausted from worrying about COVID-19 for, as Blancaneaux says, what feels like forever—learning that their families are unvaccinated, or failing to take other precautions, is a bitter pill to swallow, and one that makes it difficult to keep going about their essential work unfazed. Indeed, a sign hanging in CHNO’s emergency-department bathroom directs staff to “wipe away tears” before returning to work. “How do you try to tell someone why they should care about the life of a child?” Alabama’s Kimberlin asks. “I don’t know.” Paul Decerbo has been a member of the Rhode Island-1 Disaster Medical Assistance Team for more than 10 years, long enough to become the squad’s commander. Three months out of each year, when there’s an emergency anywhere in the U.S., Decerbo knows he may have to prepare himself and a team of on-call medics, nurses and doctors to ship out to the scene of the crisis for two weeks. Sometimes, that’s the site of a natural disaster. For the last 18 months, it’s mostly been wherever COVID-19 cases are surging and local hospitals are at their breaking points. Decerbo deployed six times last year. But when he got a call from CHNO this summer, asking for people who could help treat emergency-department patients, he faced a new challenge. He’d need an entire team of people ready to treat COVID-19 patients and trained in pediatrics—something not required during prior coronavirus surges, when the vast majority of patients were adults. Ultimately, he had to look beyond Rhode Island and assemble a squad of health-care workers from multiple states to meet that need. 
CHNO’s resident staffers weren’t quite prepared for the uptick in pediatric cases, either. “It was a shock,” Blancaneaux says. After a year of few-and-far-between cases in the pediatric hospital, “All of a sudden, eight out of the 20 patients I saw [in a day] were COVID positive.” It’s gotten to the point, he says, where doctors assume any patient who comes in with flu-like symptoms has COVID-19. The hospital’s quiet atmosphere hides the work happening behind the scenes to keep pace with that increase. CHNO has implemented an incentive program to encourage current staff nurses to pick up extra shifts, and has hired about 150 new nurses to help manage the patient load. https://datawrapper.dwcdn.net/eSb5K/3/ Perhaps more concerning, the current spike began in July, before most schools in Louisiana had started back up. As the school year continues, Delta will almost undoubtedly find new footholds. No one wants to consider what happens if this is the ascent of a bell curve, rather than the peak—particularly since vaccines for the youngest Americans may not be available until late 2021 or early 2022. Even once the shots are authorized, children too young to consent to treatment will be reliant on their parents’ willingness to get them vaccinated. That’s a troubling prospect since, in a recent Kaiser Family Foundation survey, only 26% of parents with kids ages 5 to 11, and 20% of those with kids younger than 5, said they would vaccinate their children right away. 
In some cases, that may be because parents still do not believe young children need to be vaccinated, considering their low odds of dying or becoming hospitalized. But there are always exceptions to rules, and they’re showing up every day in pediatric ICUs. Jordan Ohlsen, a nurse who works on CHNO’s acute-care floor, says some parents don’t realize how serious the virus can be until their child is the one in a hospital bed. “Once the child does get sick, their [parents’] conception of what the virus is [changes],” Ohlsen says. “When they come in and see their kid sick, in their brain it switches to, ‘This is something I should be worried about,’ or ‘I should have gotten them vaccinated.’” If there is any optimism buried within the current pediatric surge, it’s that perhaps some parents will have that realization before their child gets sick, rather than after. But with vaccine authorization for young children at least a few months away, the immediate battle is in convincing adults to get their shots, thereby hopefully driving down the total amount of virus circulating in each community. Delta seems to be scaring at least some holdouts into action. On average, more than 700,000 people in the U.S. are now getting a COVID-19 vaccine each day, a higher number than the country has reported since June. But there’s a long way to go, and not a lot of time to travel it. Particularly in areas where infection rates are high, health officials must encourage people to go back to basics, the AAP’s O’Leary says. New Orleans, for its part, has reimplemented mask mandates and now requires proof of vaccination or a negative test from anyone who wants to visit an indoor bar, restaurant or music venue, lending a somewhat subdued air to many parts of the usually buoyant city. “Use the mitigation measures we know work,” O’Leary says. “Wear masks when you’re around other people, particularly in enclosed spaces….Avoid places where lots of people are congregating.” 
Unless and until health officials can convince a tired and disillusioned populace to return to precautions they wanted to leave in the past, COVID-19 will keep spreading. A small number of patients, no matter how young, will land in the hospital. And day after day, health care workers will don their gas-mask-like respirators, gowns and goggles to care for them, many worrying all the while about bringing COVID-19 home to their own children. The staff at CHNO makes a valiant effort to stay positive and keep smiling beneath their masks—a trait, perhaps, of choosing to work in pediatrics. But Blancaneaux admits it can be difficult this far into a pandemic, when the tools for ending it are in nearly every drugstore in the country. “Everyone is frustrated and worn out and upset,” he says. “You feel unsupported by the public because we keep fighting against it. And a large part of it is preventable.” —With reporting by Emily Barone from https://ift.tt/38imR3j Check out https://takiaisfobia.blogspot.com/ (NEW YORK) — Half of American workers are in favor of vaccine requirements at their workplaces, according to a new poll, at a time when such mandates gain traction following the federal government’s full approval of Pfizer’s COVID-19 vaccine. The poll from The Associated Press-NORC Center for Public Affairs Research shows that about 59% of remote workers favor vaccine requirements in their own workplaces, compared with 47% of those who are currently working in person. About one-quarter of workers — in person and remote — are opposed. The sentiment is similar for workplace mask mandates, with 50% of Americans working in person favoring them and 29% opposed, while 59% of remote workers are in favor. About 6 in 10 college graduates, who are more likely to have jobs that can be done remotely, support both mask and vaccine mandates at their workplaces, compared with about 4 in 10 workers without college degrees. Christopher Messick, an electrical engineer who is mostly working from home in Brunswick, Maryland, said he wrote to his company’s human resources department to ask that employees be required to get vaccinated before they are recalled to the office. Messick, who is vaccinated, said he doesn’t just worry about his own health. He said he also doesn’t want to worry about getting a breakthrough infection that could land an unvaccinated co-worker in the hospital. “I don’t want sit an office for eight hours a day with someone who is not vaccinated,” said Messick, 41. “The people who are anti-vax, I see them as selfish.” So far, many vaccine requirements are coming from private companies with employees who have mostly been able to work from home during the pandemic. The companies, including major tech companies and investment banks, have workforces that are already largely vaccinated and consider the requirement a key step toward eventually reopening offices. Goldman Sachs joined that trend Tuesday, telling employees in a memo that anyone who enters its U.S. offices must be fully vaccinated starting Sept. 7. In contrast, few companies that rely on hourly service workers have imposed vaccine mandates because the companies are concerned about losing staff at a time of acute labor shortages and turnover. Exceptions include food processing giant Tyson Foods and Walt Disney World, which reached a deal this week with its unions to require all workers at its theme park in Orlando, Florida, to be vaccinated. The AP-NORC poll was conducted before the FDA granted full approval of Pfizer’s vaccine, which some experts and employers are hoping will persuade more people to get the shot and support mandates. Drugstore chain CVS said this week that pharmacists, nurses and other workers who have contact with patients will have to be inoculated, but the company stopped short of requiring the vaccine for other employees such as cashiers. The AP-NORC poll showed high support for vaccine mandates among those who say they work in person in a health care setting, with 70% approving of vaccine requirements at their workplace. The poll also showed divisions along racial lines. Seventy-three percent of Black workers and 59% of Hispanic workers — who are more likely than white workers to work in front-line jobs — support mask mandates at their workplaces, compared with 42% of white workers. In addition, 53% of Black and Hispanic workers support vaccine mandates at their workplaces, as do 44% of white workers. 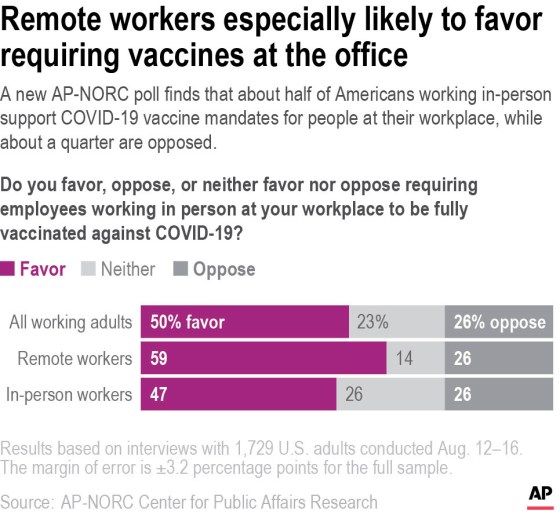
Despite mixed support for mandates among in-person employees, 71% of those workers said they themselves are vaccinated. Mike Rodriguez, a maintenance worker at an auto dealership in Florida, said he got the vaccine in the spring after a diabetes diagnosis gave him a sense of urgency. But he said he leans against supporting a vaccine mandate at his job and does not mind that masks are not required. “I don’t like being told what to do. Never have,” said Rodriguez, 54. “I’m going to wear mine no matter what. Just like whenever I go into a store. That’s my choice.” Many large retailers, grocery store chains, food manufacturers and other companies have aggressively encouraged vaccinations with bonuses, time off, information campaigns and on-site vaccination access. Janet Haynes of Topeka, Kansas, an education consultant who works part time as a package handler at a warehouse, said she struggled in March to get an appointment, putting herself on various waiting lists before she finally got a call. Now that vaccines are widely available, Haynes said she is frustrated with people who are reluctant to get them and she would support a requirement at her warehouse, where she dodges co-workers who flout a mask rule. “We get so hung up on democracy and freedom, but the reality is that your freedom can’t exist at the expense of someone else’s loss,” said Haynes, adding that she recently had a breakthrough case of COVID-19 and credits the vaccine for her swift recovery. “We are not going to be free until we get vaccinated.” ____ The AP-NORC poll of 1,729 adults was conducted Aug. 12-16 using a sample drawn from NORC’s probability-based AmeriSpeak Panel, which is designed to be representative of the U.S. population. The margin of sampling error for all respondents is plus or minus 3.2 percentage points. from https://ift.tt/3kqAHXc Check out https://takiaisfobia.blogspot.com/ It’s hard to move through the modern world without carrying a full deck of personal cards with you: driver’s license, insurance card, credit cards, bank card, Medicare card, student ID card and more. They are the transactional visas of contemporary life and they’ve been designed with that role in mind—durable, portable, easy to use, hard to forge. The newest addition is the U.S. Centers for Disease Control and Prevention’s COVID-19 vaccination card—and it violates almost every rule of good design: it’s made of perishable paper; it’s too big to fit in most wallets; it’s entirely analog—with small spaces for handwritten entries, which can be hard to read at best and entirely illegible at worst; it’s black and white and thus a cinch for forgers; it’s unencrypted—with information displayed on the face of the card rather than hidden in a QR or barcode—meaning that if you do misplace it, your health information is out in the world. What’s more, the card connects to no central database, making it impossible to link electronically with any of your other medical records. “The CDC was required to move quickly and address many complexities,” says Sandy Speicher, the CEO of IDEO, a global design firm. “There’s a need for privacy, security and accuracy and there’s a need for people to understand what this card is for and how they will use it in their lives.” The current card doesn’t really achieves any of these goals, so we asked several graphic artists to come up with alternative ideas that would respond to the 21st century scourge that is COVID-19 with a 21st century vaccination card. All of the designers believed the card should be smaller, and two of the four designed them from plastic. Not only does that make the card less destructible and easier to carry, it also serves a certain psychological function, giving it the feel of just one more card in the stack we already carry. For example, Leana Macaya, a Brooklyn-based multidisciplinary artist, designed a hard plastic card the size of a credit card, with QR codes that enable easy scanning: 
“It’s important to consider the user experience overall,” says Speicher. “The credit card is a good analogy here. Every time a restaurant or sports venue asks for proof of vaccination, that’s a health care transaction. You’re submitting your vaccine information in exchange for access.” Aesthetics matter too. Adding color to the card not only makes it harder to counterfeit, says Agyei Archer, a graphic designer based in Trinidad and Tobago, but also makes it easier to identify and distinguish at a glance. The front of Archer’s card features the CDC logo in blue and the reverse is royal blue with bold white lettering. His card is also foldable, with two interior sides that provide six spaces for listing every vaccine and booster received. That allows for easy reading of vaccine history without having to scan the card, but hides that personal data on the interior faces. A portable, plasticized card could include raised or Braille lettering—as it does on Archer’s design—for the visually impaired: Exterior faces: 

Interior faces: 

St. Louis-based illustrator Carlos Zamora took the color idea a step further, decorating the back of his version of the card with a multicolor V (for “vaccine”), along with the card-holder’s name and ID number, and using the front for playful—and brightly colored—messages. In one version, he features a pair of stylized lips with the message “Kiss Me. I’m Corona Free.” In another, he depicts the planet Earth being vaccinated, with the words “Breathe again. We are all in this together.” 
Zamora reiterates the need for a unified, electronic tracking system. “I’m basically proposing a simplified card connected to a database like a credit card and a space for public messaging to educate and promote vaccination,” he says. Using a bar or QR code to carry information like the manufacturer of the vaccine administered, the number of shots the person has received and where they got vaccinated not only helps keep confidential medical information confidential, but could also enable the authenticity of the card to be confirmed at a swipe—and to, theoretically, tell the cardholder that it’s time for, say, a booster shot or a checkup. Of course, that would require that a nationwide network of card readers similar to payment terminals were installed at venues where vaccine status would need to be confirmed—a heavy lift, but one that could pay big dividends. With nearly 86% of physicians offices now using electronic medical records, according to the U.S. Centers for Disease Control and Prevention, vaccine data collected by such a system could flow smoothly into a patient’s overall health files. “The real challenge is not just designing a card with a single piece of health data,” says Speicher, “but designing a system that gives us access to our information, and makes it easily accessible to share with the institutions we interact with—airlines, schools, restaurants, movie theaters. The system has to work well and be trusted in all directions.” Los Angeles-based designer Elisa Wong kept things simple—opting for a card that would be filled out manually and does not have a QR or barcode. What it has is wallet-sized portability and a colorful look, along with being easier and cheaper to manufacture. None of these changes would make for a perfect card, but all of them would decidedly make for a better card. For now it does appear we’re stuck with the cards we’ve got. (The CDC did not return an inquiry from TIME asking if it has plans to issue improved cards in the future.) Still, the lessons from this pandemic—and from this iteration of vaccine cards—could mean better things to come when the next health crisis hits. from https://ift.tt/3DmwDzK Check out https://takiaisfobia.blogspot.com/ Televisits for medical care took off during the worst days of the pandemic, quickly becoming commonplace. Throughout, it’s probably seemed like it doesn’t matter what state the provider of these telehealth services is located. But that’s only because most states, along with the U.S. Centers for Medicare & Medicaid Services, temporarily waived rules requiring licensed clinicians to hold a valid license in the state where their patient is located. Now states are rolling back many of those pandemic workarounds—meaning the ability to conduct certain virtual appointments may be nearing an end. Johns Hopkins Medicine in Baltimore, for example, recently scrambled to notify more than 1,000 Virginia patients that their telehealth appointments were “no longer feasible,” says Dr. Brian Hasselfeld, medical director of digital health and telemedicine at Johns Hopkins. Virginia is among the states where the emergency orders are expiring or being rolled back. Only about 17 states still have waivers in effect, according to a tracker maintained by the Alliance for Connected Care, a lobbying group representing insurers, tech companies and pharmacies. As those rules end, “it risks increasing barriers” to care, says Hasselfeld. Johns Hopkins, he adds, hosted more than 1 million televisits, serving more than 330,000 unique patients, since the pandemic began. About 10% of those visits were from states where Johns Hopkins does not operate facilities. The rollbacks come amid a longer and larger debate over states’ authority around medical licensing that the pandemic—with its widespread adoption of telehealth services—has put front and center. “Consumers don’t know about these regulations, but if you all of a sudden pull the rug out from these services, you will definitely see a consumer backlash,” says Dr. Harry Greenspun, chief medical officer for the consultancy Guidehouse. Why cross-state telehealth is an issue to begin withFinding a way forward pits high-powered stakeholders against one another, and consumers’ input is likely to be muted. Barak Richman, a Duke University law professor argues that laws and policies haven’t been updated to reflect new technological realities partly because state medical boards want to hang onto their authority. These state boards say their power to license and discipline medical professionals boosts patient safety. Licensing is also a source of state revenue. Providers have long been split on whether to support changing cross-state licensing rules. Different state requirements—along with fees—make it cumbersome and expensive for doctors, nurses and other clinicians to get licenses in multiple states, leading some to call for more flexibility. Even so, those efforts have faced pushback from within the profession, with opposition from other clinicians who fear the added competition that could come from telehealth could lead to losing patients or jobs. “As with most things in medicine, it’s a bottom-line issue,” says Greenspun. “The reason telehealth has been blocked across state lines for many years related fundamentally to physicians wanting to protect their own practices.” But the pandemic changed the equation. Even though the initial spike in telehealth visits has eased, use of the services has stabilized at levels 38 times higher than before the pandemic, according to a July report from consulting firm McKinsey and Co. Patients’ experience with televisits coupled with the growing interest by investors is focusing attention on this formerly inside-baseball issue of cross-state licensing. Meanwhile, patients and their doctors are getting creative, with some simply driving across state lines, then making a Zoom call from their vehicle. “It’s not ideal, but some patients say they are willing to drive a mile or two and sit in a parking lot in a private space and continue to get my care,” says Dr. Shabana Khan, director of telepsychiatry at NYU Langone Health’s department of child and adolescent psychiatry. She and other practitioners ask their patients about their locations, mainly for safety reasons, but also to check that they are in-state. Other patients, of course, are seeing telehealth care providers many miles away, so driving to another state for a virtual appointment will not ever be a realistic option. Khan worries about people whose care is interrupted by the changes, especially those reluctant to seek out new therapists or who cannot find any clinicians taking new patients. Austin Smith hopes that doesn’t happen to him. After initial treatment for what he calls a “weird flavor of cancer” didn’t help reduce his gastrointestinal stromal tumors, he sought out other options and eventually landed in a clinical trial for a drug to treat his cancer. But it was in San Diego and the 29-year-old salesman lives in Phoenix. Although he drives more than five hours each way every couple of months for treatment and to see his doctors, he does much of his other follow-up online. And if the rules change? It will mean a lot of inconvenience and time on the road for him compared to his current on-line follow up care but he’ll keep making the drive. “I’ll do anything to beat this,” he says of his cancer. Where doctors standBut will doctors, whose patients have spent the past year or more growing comfortable with virtual visits, also be willing to take steps that could likely involve extra costs and red tape? For instance, submitting license applications in another state can take weeks or even months. They must pay application fees and then have to keep up with a range of ongoing requirements such as continuing education, which vary by state. States boards say their traditional role as medical practitioner overseers ensures that all applicants meet educational requirements and pass background checks. They also investigate complaints and argue there’s an advantage to keeping local officials in charge. “It’s closer to home,” says Lisa Robin, chief advocacy officer with the Federation of State Medical Boards. “There’s a remedy for residents of the state with their own state officials.” Some doctor groups, such as the American Medical Association, agree. Allowing a change that removes centralized authority from a patient’s home state would raise “serious enforcement issues as states do not have interstate policing authority and cannot investigate incidents that happen in another state,” said then-AMA President-elect Jack Resneck during a congressional hearing in March. But others want more flexibility and say it can be done safely. Hasselfeld, at Johns Hopkins, says there is precedent for easing multistate licensing requirements. The Department of Veterans Affairs, for example, allows medical staffers who are properly licensed in at least one state to treat patients in any VA facility. The Alliance for Connected Care and other advocates are pushing states to extend their pandemic rules. A few have done so. Arizona, for example, made permanent the rules allowing out-of-state medical providers to practice telemedicine for Arizona residents, as long as they register with the state and their home-state license is in good standing. Connecticut’s similar rules have now been stretched until June 2023. Advocates also call for the federal government to enact more sweeping changes, and back legislation pending in Congress that would temporarily allow medical professionals licensed in one state to treat—either in person or via televisits—patients in any other state. The working models for a future systemBecause such fixes are controversial, voluntary interstate pacts have gained attention. Several already exist: one each for nurses, doctors, physical therapists and psychologists. Proponents say they are a simple way to ensure state boards retain authority and high standards, while making it easier for licensed medical professionals to expand their geographic range. The nurses compact, enacted by 37 states and Guam, allows registered nurses with a valid license in one state to have it automatically recognized by all the others in the pact A different kind of model is the Interstate Physician Licensure Compact, which has been enacted by 33 states, plus the District of Columbia and Guam, and has issued more than 21,000 licenses since it began in 2017, says Robin, of the Federation of State Medical Boards. While it speeds the paperwork process, it does not eliminate the cost of applying for licenses in each state. The compact simplifies the process by having the applicant physician’s home state confirm his or her eligibility and perform a criminal background check. If the applicant is eligible, the home state sends a letter of qualification to the new state, which then issues a license. To be eligible, physicians must meet all rules and laws in each state, such as requirements for continuing medical education. Additionally, they cannot have a history of disciplinary actions or currently be under investigation. “It’s a fairly high bar,” says Robin. Such compacts—especially if they are bolstered by new legislation at the federal level—could help the advances in telehealth made during the pandemic stick around for good, expanding access to care for both mental health services and medical care across the U.S. “What’s at stake if we get this right,” says Richman at Duke, “is making sure we have an innovative marketplace that fully uses virtual technology and a regulatory system that encourages competition and quality.” KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. from https://ift.tt/3kvrWev Check out https://takiaisfobia.blogspot.com/ Americans have reached consensus on a single goal: children must return to classrooms. Yet, as the Delta variant has surged, policymakers across the country have abandoned measures to protect unvaccinated children from COVID-19. Months after a withering debate on the best way to open schools, only 12 states have school mask mandates while 9 have banned them. In Florida, Gov. DeSantis signed an executive order prohibiting mask mandates in schools, and the State Board of Education threatened to withhold state funding from districts that required masking in defiance of his prohibition. Several governors, including Tennessee’s Bill Lee, have issued orders allowing parents to opt out of local mandates. Even in Vermont, a state lauded as a model for its approach to school reopening and vaccination rates, children have been an afterthought of the pandemic response. As a public health researcher, practitioner, and parent in Vermont, I’ve watched the state over the last year retreat from many of the lessons it initially offered for a country struggling to return children to classrooms. Vermont reopened its schools on September 8, 2020 with robust, 41-page statewide guidance amid a mere 5 cases. State and school leaders called upon communities to come together to keep kids safe and in-school. When cases flared in late fall, Vermont Governor Phil Scott closed bars and instituted restrictions on social gatherings, travel, and sports. Keeping kids in school represented a central priority for the state, and leaders aligned its public health response to achieve this goal. Yet, Vermont’s state leadership has set aside key elements of its success as it has prepared for the 2021-22 school year. Citing its high vaccination rates, the state bucked CDC and AAP masking guidance in its 1.5 page reopening memo recommending “light touch” mitigation measures in K-12 schools even as it in August registered the fastest growing epidemic in the U.S. State leaders recommended masking in children under 12 and in students 12 and older in schools with vaccination rates less than 80% but stopped short of mandating it. Absent in state plans were descriptions of the robust layered approach including effective ventilation that experts widely view as essential to reopening as the hyper-transmissible Delta variant spreads. Vermont’s local control approach has left school leaders and unvaccinated children at the mercy of village political whims and expertise. School leaders struggle to make public rapidly changing conditions, and some report receiving threats from community members opposed to mask requirements. Schools in the country’s most vaccinated communities have adopted the CDC and American Academy of Pediatrics (AAP) guidance in full while the school board in Essex County, an area with vaccination rates more than 25% lower than the rest of the state, voted 5-0 against masking. As a result, some unvaccinated Vermont children will return to schools with more limited mitigation measures in place than what the CDC recommends in public indoor settings in counties with substantial or high transmission. Yet, the risk of a variant twice as transmissible as the wild-type virus is far greater this fall and therefore calls for redoubling mitigation strategies. Gov. Scott is not the only governor hiding behind the state’s high vaccination rate and counterparts who have shown outright disregard for the health and education of children. Once criticized for instituting an outdoor masking mandate, Massachusetts Gov. Baker rejected calls from the Massachusetts Medical Society, Teachers’ Unions, and others for universal masking mandates in schools, leaving the onus of public health decision making on the state’s 404 individual school boards. New Hampshire Gov. Sununu signed a law banning vaccine mandates while eschewing calls for masks in schools. These actions have come at the most dangerous moment for children in the pandemic. Children now account for nearly 1 in 5 cases of COVID-19 in the U.S, and pediatric Covid-19 hospitalizations have reached their pandemic record. Schools that have opened without mitigation measures in place now have sent thousands of students into quarantine within days, and staff shortages have forced others to close. Even as vaccines continue to protect against hospitalizations and death, mounting data highlights the imperative to employ robust strategies to protect children too young to be vaccinated. It’s time to stop minimizing the risk of Covid-19 to children and debating minimalistic approaches to reopening schools. U.S. and state leadership must build on the best practices from Vermont and other states, rather than rationalizing policy choices that compromise the health and education of children mere weeks or months before they are eligible for vaccination. Heavily vaccinated states such as Vermont must once again lead by example and use all available tools to ensure a safe return to in-person education. Returning children safely to classrooms must now be the central goal of the public health response. To this end, governors must institute indoor mask mandates—and restrict other activities as conditions dictate–to curb skyrocketing cases across communities. At the same time, governors must mandate robust school guidance that employs all evidence-based tools to keep kids healthy and in school, including universal masking, ventilation, testing, and controls on high-risk indoor activities, including lunches. States must also ensure that students with high-risk medical conditions have access to remote learning or other accommodations until they are eligible for vaccination. Vermont has taught the country that it takes a village to bring children back to school during a pandemic, but now we must not leave villages to manage the pandemic on their own. Instead, the U.S. must center the health and education of its children in a unified public health response and create the conditions for a safe return to schools. from https://ift.tt/3knH6Cz Check out https://takiaisfobia.blogspot.com/ (ATLANTA) — A few weeks into the new school year, growing numbers of U.S. districts have halted in-person learning or switched to hybrid models because of rapidly mounting coronavirus infections. More than 80 school districts or charter networks have closed or delayed in-person classes for at least one entire school in more than a dozen states. Others have sent home whole grade levels or asked half their students to stay home on hybrid schedules. The setbacks in mostly small, rural districts that were among the first to return dampen hopes for a sustained, widespread return to classrooms after two years of schooling disrupted by the pandemic. In Georgia, where in-person classes are on hold in more than 20 districts that started the school year without mask requirements, some superintendents say the virus appeared to be spreading in schools before they sent students home. “We just couldn’t manage it with that much staff out, having to cover classes and the spread so rapid,” said Eddie Morris, superintendent of the 1,050-student Johnson County district in Georgia. With 40% of students in quarantine or isolation, the district shifted last week to online instruction until Sept. 13. More than 1 of every 100 school-aged children has tested positive for COVID-19 in the past two weeks in Georgia, according to state health data published Friday. Children age 5 to 17 are currently more likely to test positive for COVID-19 than adults. Around the country, some schools are starting the year later than planned. One district in Western Oregon pushed back the start of classes by a week after several employees were exposed to a positive teacher during training. Before the latest virus resurgence, hopes were high that schools nationwide could approach normalcy, moving beyond the stops and starts of remote learning that interfered with some parents’ jobs and impaired many students’ academic performance. Most epidemiologists say they still believe that in-person school can be conducted safely, and that it’s important considering the academic, social and emotional damage to students since the pandemic slammed into American schools in March 2020. In some cases, experts say, the reversals reflect a careless approach among districts that acted as if the pandemic were basically over. “People should realize it’s not over. It’s a real problem, a real public health issue,” said Dr. Tina Tan, a Northwestern University medical professor who chairs the American Academy of Pediatrics Section on Infectious Diseases. “You have to do everything to prevent the spread of COVID in the school.” Tan and others say that means not just masks in schools but a push for vaccination, social distancing, ventilation and other precautions, providing multiple layers of protection. Dairean Dowling-Aguirre’s 8-year-old son was less than two weeks into the school year when he and other third graders were sent home last week in Cottonwood, Arizona. The boy took classes online last year and was overjoyed when his parents said he could attend school in-person. But Dowling-Aguirre said she grew more anxious as infections climbed. Masks were optional in her son’s class, and she said fewer than 20% of students were wearing them. Then she got a call from the principal saying her son had been exposed and had to stay home at least a week. Of particular concern was that her parents watch her son after school and her mother has multiple sclerosis. “It’s definitely a big worry about how it’s going to go from here on in and how the school’s going to handle it,” she said. In Georgia, more than 68,000 students — over 4% of the state’s 1.7 million in public schools — are affected by shutdowns so far. Many superintendents said they have already recorded more cases and quarantines than during all of last year, when most rural districts held in-person classes for most students. “This year, you saw it very quickly,” said Jim Thompson, superintendent in Screven County, Georgia. “Kids in the same classroom, you’d have two or three in that classroom.” Thompson said the county’s 25-bed hospital warned it was being overloaded by infections but what led him to send the district’s 2,150 students home was concern that he wouldn’t be able to staff classes. “You don’t want to start the school day and find you don’t have enough teachers,” Thompson said. The onslaught is driving changes in mask policies. Weeks before school started, only a handful of large districts covering fewer than a quarter of students across Georgia were requiring face coverings. Now, mask mandates cover more than half of students. Part of the mask policy change is driven by a shift in U.S. Centers for Disease Control and Prevention guidance. The CDC now advises that when everyone is wearing masks, exposed students 3 feet (1 meter) or more apart don’t have to be sent home if they’re not showing symptoms. Angela Williams, the superintendent in Burke County, Georgia, said she believes masks and that rule will allow her 4,200-student district near Augusta to avoid further disruptions after its current two-week shutdown. “That is going to cut down on the number of students we’re having to quarantine,” Williams said. Georgia told districts in early August that they could choose their own quarantine policy, and some loosened rules. Thompson, though, said Screven is likely to retighten its policy when it returns and require everyone who is exposed to quarantine for at least a week because of delta’s high contagion level. “We started with utilizing that latitude to its fullest,” Thompson said. “That did not work for us locally.” Some districts are also looking to boost vaccination rates among staff and eligible students, but most Southern schools appear unlikely to mandate teacher vaccination or testing, unlike states on the West Coast and in the Northeast. Thompson said he sought to schedule a vaccine clinic in Screven County last week but got so few takers it was canceled. Despite disruptions, there’s still strong resistance to masks. In the 28,000-student Columbia County in suburban Augusta, officials said they were putting plexiglass dividers back up in school cafeterias, as well as limiting field trips, school assemblies and classroom group work. But the district continues to only “strongly recommend” masks. Even some districts that have sent all their students home don’t expect to require masks when they return, facing opposition from parents and the school board. “They wanted that that should be the parents’ decision,” Morris said of school board members. from https://ift.tt/3B8bWpt Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
