|
Spirits are high as the students file into the basement of the Galante Funeral Home in Union, N.J., to pick out their caskets. Jessica Polynice, 23, beelines toward the most ornate one in the showroom, joking that she has expensive taste. Others consider the prominently displayed price tags, from $995 to nearly $6,000, and factor in the softness of the pillows. Surrounded by open caskets, Amanda Davis, 20, says she’d rather be cremated into a firework. Beside her, Lauren Duffy, 24, flips through a brochure for artificial reef cremations and weighs whether she’d like to be eternally memorialized on the ocean floor. The decisions, largely hypothetical, are all part of their next homework assignment to plan their own funerals, presumably for the very far future. They’re among 60 students taking Kean University’s Death in Perspective course this semester, which is one of the many college classes on death and dying in the U.S. that have grown in popularity during the pandemic. And it’s become much more of a grief-support group, professor Norma Bowe says, which is why the field trip to the funeral home starts off lighthearted but ends in tears. Read more: Death Doulas Used to Be Rare. The COVID-19 Pandemic Changed That <strong>“We study dying to know how to live.”</strong>In the last 30 minutes, grief that was well hidden in the funeral home basement pours out of the students in the sitting room upstairs as they share farewell letters they’ve written posthumously to people they’ve lost. “I still feel you at the house,” one student tells her stepfather, who died in 2019 in a suspected suicide. “You’re everywhere there and nowhere at all.” Other letters are addressed to a grandfather whose cancer was caught too late, a 4-year-old cousin killed by a car, a brother lost to drug abuse, an unborn child. 
“People are coming to this class to lay down their grief,” says Bowe, who gives extra credit to anyone who cries. There’s now a four-year waiting list to enroll in her class. At DePaul University in Chicago, Craig Klugman says there’s been “more buzz” recently about his course on death than in any of the past seven years he’s taught it. And a rise in interest in Duke University’s death-and-dying course has been significant enough that professor Deborah Gold kept teaching it, even though she officially retired earlier that summer. After doubling the number of annual course offerings, Gold still can’t meet the demand. ‘These kids are scared’Nationwide, students are clamoring to study death from all angles—philosophically, biologically, sociologically, and historically—at ages when most people see themselves as invincible. But it’s not morbid curiosity or grim fatalism at work. Grief is surging among college students, and many are shouldering multiple losses during the pandemic, according to a study published last year in OMEGA–Journal of Death and Dying. While the most common reported loss was of a sense of normality, the study found that more than 10% of the college students surveyed said a loved one had died of COVID-19. More than 26% said someone close to them had perished for other reasons. In the face of endless death, classes and other experiences that bring death into focus have become an outlet for young people to process their grief, manage their fears of dying, and reckon with their own mortality. “These kids are scared,” Gold says. “They belong to the age group that believes they are immortal, and all of a sudden it’s not so true anymore.” 
For decades, death has been mostly viewed as a taboo subject that most people would rather avoid until it became unavoidable. But young people in the U.S. today can’t escape the fact that from 2019 to 2020, the nation’s life expectancy saw its biggest one-year drop since World War II, mainly because of COVID-19. And after rampaging through older generations, the virus is now affecting younger people in higher numbers than ever before. While death among young people remains low relative to death rates for their elders struck by COVID-19, people ages 18 to 29 now account for the biggest increase in virus cases, according to the latest data from the U.S. Centers for Disease Control and Prevention. “Seeing so many people my age dying,” Polynice says, “it scares the hell out of me.” Add to the mix a gloomy forecast for the planet as climate change spawns lethal weather events, as well as iffy career prospects upon graduation, and it’s clear that COVID-19 isn’t the only anxiety crippling young Americans. “This generation of college students—they’re experiencing cumulative losses in a way that really is unprecedented in our lifetime,” says Erica H. Sirrine, the lead author of the grief study and the director of social work at St. Jude Children’s Research Hospital. Read more: Funeral Costs Are Driving Families Hit by COVID-19 to Desperate Measures That’s changed the way many people deal with the inevitable. For the first time, according to one survey, people ages 18 to 34 are 16% more likely to have a will than those ages 35 to 54. The younger generation was the most likely to cite COVID-19 as a major reason to plan for death, the survey said. And while people 55 and older are less likely to have a will than in pre-pandemic years, younger Americans are now 63% more likely to have one. “For the first time in a generation, everyone is experiencing the possibility that death may touch their lives—not someday, but now,” says Ann Burns, president of the American College of Trust and Estate Counsel. <strong>“Seeing so many people my age dying, it scares the hell out of me.”</strong>Others are looking for answers in rather unlikely places: college classrooms. Kiara Pauli, 21, experienced her first world-shattering death on Dec. 7, 2020, when her 15-year-old brother was fatally shot. “I felt like I was drowning in my anger and confusion,” she says. Her trauma was compounded by the increasing nationwide death toll from COVID-19, which exacerbated her fear of dying. Pauli, who had never had to deal with death, was suddenly surrounded by it. 
In September 2021, she took a death-and-dying class at DePaul—the first time she had forced herself to think about death for a prolonged period of time. Pauli’s perspective changed the first day, when she and about 30 other students watched a video of an elderly man dying, surrounded by loved ones. Klugman, who designed the course, says he uses the video to show what a peaceful death looks like, since most students have never seen someone die. “The first day is about normalizing death and recognizing that at least in the U.S., most people have some anxiety about it,” he says. The video showed Pauli that dying isn’t always terrifying or painful. Read more: Children and Teenagers Are Being Shot in Record Numbers One month later, Pauli’s grandfather died following a heart attack. The college junior clung to the lessons she had just learned. She told herself he did not suffer at the end because, thanks to the video of the elderly man, she now had a better understanding of what might happen to someone in their final moments. By the time the course was over in November, Pauli realized she was scared of dying because she didn’t want to be forgotten. She decided to become an author to leave behind a physical legacy. “We study dying to know how to live,” she says. “The class was like the near-death experience that makes people figure out priorities.” How death classes fill a role that counseling cannotIn the past two years, college death classes have become one of the most available and affordable options that some students have to deal with their grief. While most U.S. universities offer counseling services to students at little or no additional cost, when campuses closed during the pandemic and learning went remote, tens of thousands of out-of-state students lost access to those services because of differing telehealth guidelines in their home states, says Dr. Ryan Patel, chair-elect of the American College Health Association’s mental-health section. A school psychiatrist or counselor in Ohio, for example, would not be able to virtually counsel, on a routine basis, a student who was home in New York, without a license in the other state. 
That left few other options for many who were struggling. They could see a therapist or another professional, which could cost $50 to $100 out of pocket for one session, depending on where they live, says Patel, who is also a psychiatrist at Ohio State University. They could also contact several free national crisis help lines. But those providers might not be as specifically trained to understand the unique academic, social, and financial struggles that young students endure as much as campus counselors might, Patel says. Even those who stayed in-state and maintained access to their college’s counseling services faced hurdles. Some, surrounded by family members at home, lost a sense of privacy to discuss their mental health, while others went back to environments that worsened their mental health. The predicament has only grown more dire amid the rapid-spreading Omicron variant. Patel worries these challenges will continue in the near future. <strong>“We carry grief like a backpack full of bricks.”</strong>“A hybrid form of education in some form is here to stay,” he says. “So we’re left with trying to figure out how we are going to provide support services for students.” 
College classes on death and dying are not new. Bowe, a registered nurse, has been teaching her course since 1997, and Gold’s class at Duke was first approved in 2001. But their rise in popularity in a pandemic makes sense from a psychological viewpoint, says Coltan Scrivner, a University of Chicago researcher who studies morbid curiosity. In a 2020 study, Scrivner found that people watched horrific things, like scary movies, as a coping mechanism during the pandemic. The study said horror fans and the morbidly curious have been more psychologically resilient as the world changed. “It feels good to control what will terrify you,” Scrivner says. Some philosophy students may find it easier to cope with death by discussing at length the possibility of an afterlife, or whether the fear of death is rational, says Yale University professor Shelly Kagan. Other students elsewhere appear to be craving concrete, scientific knowledge. At DePaul, Klugman has noticed a new surge in interest from students with questions about infectious diseases. In 2020, he added a new lecture comparing COVID-19 to past pandemics like the 1918 flu, and other mass deaths from major natural disasters. “What they want to know has changed,” Klugman says. His students frequently ask how to talk to somebody who has lost a loved one and, more specifically, how to talk to someone who has lost a loved one to COVID without getting into a political argument. 
For many, a mental-health necessityBowe has seen a similar shift. Three years ago, she’d say her students were drawn to her class for the unique field trips, which got them out of school to watch live autopsies at morgues and roam cemeteries for scavenger hunts in the evenings. Today, those trips are only minor perks, and the class itself has become more of a mental-health necessity. “We carry grief like a backpack full of bricks,” Bowe says. “There’s nowhere to let it go.” The recent funeral-home trip exposed just that. Many of the students’ wounds were fresh, but several have never healed. Polynice has been suffering in silence for nearly a decade. Her family avoids talking about her grandfather’s traumatic death, so she’s not used to acknowledging the pain she still feels. And while she made jokes as she shopped for caskets, tears welled in her eyes as she revealed she was 14 when her grandfather bled to death in the home they shared. He had accidentally hit a tube kept in his arm for dialysis treatments, Polynice says, adding that she remembers waking up to screams and cries. “This class makes you uncomfortable,” she says, “but I’m better because I’m able to talk more openly about it.” <strong>“No one teaches you how to grieve.”</strong>Amanda Davis, whose 78-year-old grandfather died over the summer from cancer that spread from his liver to his bones, has gotten the same sense of closure. “No one teaches you how to grieve,” says the sophomore from Sacramento, who is one of the first volunteers to share her farewell letter with the class. “Things remind me of you every day,” she reads out loud, turning bright red as her face mask absorbs the falling tears. But as soon as she’s done, Davis feels instant relief. 
In the past two years, all 330 students who have taken Bowe’s death class have either lost a loved one to COVID-19, know somebody who has, came close to losing someone to the virus, or almost died from it themselves. The disease took two from Daniela Derius-Rodriguez, just as she was about to complete Bowe’s course. After being put on a ventilator, Derius-Rodriguez’s mother died on April 21, 2020, three weeks after the student’s grandfather had died. At 21, it was the first time she had experienced death. “I was grieving while learning about grieving,” she says. Bowe said that she didn’t have to finish out the semester, that she had already gotten an A. It didn’t matter to Bowe if Derius-Rodriguez took the final exam, which consists only of reflective questions, because her main goal as a death-class professor is for every student to walk away with a deeper appreciation of life. But Derius-Rodriguez still came to class and handed in every assignment until she graduated that May. Her grandfather and mother had always put an emphasis on education and the importance of working through hardships, so Derius-Rodriguez didn’t want to take the easy way out. But she had also come to rely on her classmates for support, and on the lessons to make sense of how she was feeling. 
“I was in a room full of strangers, but I felt so connected to them,” she says. The class kept her from being closed up, and she made sure the rest of her family wasn’t bottling up their pain too. Without the class, she says, “I would have been in the dark.” At a minimum, death classes get people talking about their pain rather than holding it in, says Sirrine, the grief-study author, who until recently had taught college death classes in Florida for the past 14 years. They also increase empathy at a time of fraught social interactions. “If we can move toward each other and extend more compassion to people who are suffering,” Sirrine says, “then maybe the pandemic won’t be all a loss.” Two years ago, when Derius-Rodriguez perused caskets at the funeral home for the first time during one of Bowe’s field trips, she crossed her fingers and hoped she’d never have to organize a funeral for real. A month later, she was helping her family plan two. The 23-year-old now understands that grief is inevitable because it’s a by-product of love. “When it does come to us,” she says, “we need to learn how to handle it.” from https://ift.tt/hGlne6p Check out https://takiaisfobia.blogspot.com/
0 Comments
Dr. Paul Farmer, a physician, medical anthropologist, and mentor to many, died on Monday in Butaro, Rwanda. Partners in Health, the organization he co-founded, confirmed his death in a tweet on Monday. He was 62. Dr. Farmer is survived by his wife, Didi Bertrand Farmer, three children, and thousands of patients and students, like myself, who honor his memory today. While messages pour out from heads of state and celebrities, it is the unified voice of grief from his colleagues and students that underscores the resounding loss felt within the field of global health. Dr. Paul Farmer was a guiding light and inspiration to thousands looking to advance the health of vulnerable people across the world. After graduating from Duke University in 1982, Farmer joined Harvard University, earning an MD and a PhD in medical anthropology. He made many trips to Haiti during these formative years, volunteering at a hospital in Cange, Haiti. Here, he helped introduce a revolutionary concept into the field of healthcare and medicine, which has progressively become a privilege of those with money, access, and other forms of power: that all people are deserving of equally excellent care. He believed, “The idea that some lives matter less is the root of all that is wrong with the world.” This led him to co-found Partners in Health in 1987 as a young medical student at Harvard Medical School, alongside Ophelia Dahl, Thomas J. White, and Jim Yong Kim. The organization succeeded in bringing high-quality care in resource limited settings such as Haiti, Rwanda, and Lesotho. Dr. Farmer didn’t just believe in the idea of health as a human right, he lived and taught those values. In a remarkable but characteristic move, Dr. Farmer maintained his role as a practicing physician throughout his career. While to those outside of medicine, this may not resonate as significant, to those of us within that circle it is an extraordinary move – moving mountains at the systemic level by leading an organization or making change in international health policy requires so much time and energy that typically physicians temporarily or indefinitely pause their clinical practice. For Dr. Farmer, it was always about changing an individual life. As Tracy Kidder, the author of Mountains Beyond Mountains, a book about Farmer, wrote, “he was a doctor first of all.” Dr. Farmer was always known for personally going on rounds in the hospital wards, letting the lived experience of patients guide him and others. To those of us that had the good fortune to be his students, Dr. Farmer was determined to bring us along his path to advance the health of all. He taught us with a passion that made it clear that the fate of individual men, women, and children rested in the care we provided. And it didn’t stop at noting a patient’s medication or writing down a diagnosis in a chart. Rather, it meant hearing their stories. As a student from 2014 to 2015 in the masters of medical anthropology program at Harvard University where Dr. Farmer taught alongside giants like Arthur Kleinman, I learned from him how biopsychosocial factors such as poverty, the environment, and public policy caused ill health. These concepts only recently have started to find their way into medical school education. At a time when medicine was about anatomy, biology, or physiology, he taught how deep poverty in Haiti might increase the deadliness of a manageable condition like HIV/AIDS, or how a lack of access to roads might prevent an individual from getting necessary tuberculosis medications. In addition to knowing what HIV/AIDS does to a person’s immune system or what antibacterial medications to give for tuberculosis, it was about understanding the real, full life story of a patient to understand their illness. “If you look at apartheid in South Africa, you see that people get sick with tuberculosis, malaria and other diseases because of poor work conditions, lack of jobs, shantytowns. You have to look at what’s happening to the patient in front of you, and think about ways to address social disparities. If there’s food insecurity, then you provide food when you provide care. Or if patients drop out of treatment, you provide transportation to the clinic, or you send community health workers to the patient,” he told NPR in a 2020 interview. He trained a generation of healthcare providers to consider these factors a critical part of health and illness, at a time when few others were making these connections for us. With his radical approach and generosity of spirit, he trailblazed a pathway for global health to be a social justice movement. Through his own work, and through the continued work of his students, he improved the life and wellbeing of countless patients across the world. As a testament to how universally beloved he was, from patients to trainees to colleagues, Dr. Farmer was the godfather to more than 100 children, most of them in Haiti. Importantly, Dr. Farmer brought this social justice movement and the care of vulnerable populations across the world to the hearts and minds of a broad audience, bringing global health back to the U.S. Through articles and 12 books he explained his vision for more equitable health to the public and helped shape a generation of doctors and healthcare providers. Bringing together health experts, government officials, and donors, he helped found the University of Global Health Equity in 2015 in Butaro, Rwanda. And he brought each person along this journey with kindness, grace, and humility. When, from Rwanda, I’d asked him for help in setting up our early partnership with the University of Global Health Equity, after resolving the situation, he replied with gratitude for our work, as though it wasn’t all there because of his vision and efforts. It is but once in a lifetime that a physician so steeped in caring, compassion, and selfless service comes along who can change not only the world for a patient, but who can change how the world understands patients. While a giant has left us, the field of global health will be carried forward by thousands of his students and countless more who have been inspired by his work, with the vision of providing equitable healthcare for all. from https://ift.tt/yx1mwdF Check out https://takiaisfobia.blogspot.com/ Maria Venetis got a breakthrough case of COVID-19 right around New Year’s Eve. When she called friends to cancel plans, she found herself overexplaining how and where she might have caught the virus—until one friend cut her off. “It doesn’t really matter,” Venetis, an associate professor of communication at Rutgers University, remembers her friend saying. In that moment, Venetis realized “there is no reason for me to point a finger about where I may have possibly gotten this.” COVID-19 is such a contagious and widespread disease that feeling guilty for contracting it is, at this point, illogical. But even with experts predicting that the virus will soon become endemic, the shame of getting it persists. Studies and anecdotal reports show that many people who test positive experience shame and guilt—perhaps because they regret accidentally exposing others, feel like failures for not doing enough to prevent it, or experience stigma online. Liat Hamama, a professor of social work at Tel Aviv University, recently researched guilt and shame among more than 300 people in Israel who tested positive for COVID-19. She found that almost 14% of study participants felt strong shame about their diagnosis and about 16% felt a lot of guilt—not the majority, but a sizable minority. Those feelings appear to be more common in the U.S. In late 2020, when Johns Hopkins researchers surveyed approximately 1,500 Americans, about 25% said they would feel ashamed if they caught COVID-19. Those feelings have clear consequences for mental health, but they could also be problematic from a public-health standpoint. The Johns Hopkins researchers linked COVID-19 stigma to a person’s reluctance to seek medical care, test, and tell others who might have been exposed. Another study, published in 2021, also found that COVID-19 shame was linked to lower compliance with public health guidelines, such as notifying health officials and close contacts. Plenty of health conditions, from sexually transmitted infections to mental health disorders, carry damaging stigma—but respiratory diseases typically don’t. “How often do people feel ashamed that they got the flu?” says Joe Gieck, an assistant professor of psychiatry and behavioral medicine at the Virginia Tech Carilion School of Medicine. COVID-19 may be different because it has shaped nearly every aspect of our lives for the past two years. The disease—along with measures used to prevent it—have also become intensely politicized, leading people to assign moral values to what should be benign public health precautions. Masking and getting vaccinated, for example, can be described as either ethical responsibilities or infringements on personal liberties, depending on a person’s perspective. In that emotionally heightened state, people are quick to call out those they perceive as behaving badly, especially on social media. “We have this built-in mechanism of trying to be good citizens, but also ostracize those who aren’t,” Venetis says. Research has repeatedly shown that shaming isn’t a good way to prompt behavior change, but people do it anyway. Risk communication has likely also contributed to perceptions of the virus. Guidance issued by public health authorities including the U.S. Centers for Disease Control and Prevention (CDC) has often focused on the actions of individuals, from the “just stay home” days of spring 2020 to more recent advice about wearing protective respirators like N95s. “There’s been so much emphasis on prevention and mitigation,” Gieck says. When someone follows all the “right” steps and gets sick anyway, “it can result in a sense of having done something wrong.” Many people are also afraid of COVID-19, and fear can exacerbate negative emotions when someone does test positive, Gieck says. Read More: COVID-19 Seems to Spare Most Kids From Illness, but Its Effect on Their Mental Health Is Deepening Guilt and shame are closely related, but not identical. “Guilt is, ‘I feel bad about what I did,’ and shame is, ‘I am bad because of what I did,’” says Sonya Norman, a professor of clinical psychiatry at the University of California, San Diego. While guilt can at least motivate people to make more conscientious decisions moving forward, shame is rarely productive, she says. Internalizing shame can be damaging to mental health and is linked to depression and low self-esteem. Shame is also associated with poor anger regulation and interpersonal problems, Hamama adds. More from TIMENorman is working on a therapeutic intervention for people who have struggled with COVID-19-related shame based on her previous work treating U.S. veterans. It guides people to recognize why they feel ashamed; addresses “hindsight bias,” or the tendency to judge past decisions based on present knowledge; and finds strategies for releasing guilt and shame in the future. Norman is still studying the program and its efficacy but says she has gotten promising feedback from patients. Not everyone can or will find a therapist to do that kind of one-on-one work, so it’s also important to address COVID-19 shame at a societal level—particularly as we prepare for a near future in which the virus is treated as an unfortunate but constant part of life. “How we talk about everything makes a difference,” Venetis says. In personal relationships, Venetis says messages like the one she got from her friend after testing positive—that it’s okay and no one’s fault—can help normalize the diagnosis. Conversely, overanalyzing where someone got COVID-19 is rarely helpful and can imply that the sick person did something wrong. Public health authorities like the CDC can use similar tactics. Jennifer Manganello, a health communications expert at the University at Albany School of Public Health, says the language used to describe COVID-19 is important. Talking about people “acquiring” or “contracting” COVID-19 is better than saying someone “transmitted” the virus or “infected” someone else, she says, because it takes blame out of the equation. It’s also important to give people actionable public-health advice while emphasizing that some things are beyond their control, Manganello says. While individuals can and should take certain precautions, like getting vaccinated and boosted, the virus continues to mutate and spread due to societal factors like global vaccine inequality. “Individual actions are just one piece of the puzzle,” Manganello says. Health communications may be most effective coming from sources whom people inherently trust, such as pediatricians and community doctors, says Dr. Scott Ratzan, founding editor of the journal Health Communication: International Perspectives. The pandemic has caused an erosion of trust in the government and public health groups like the CDC, but most people still trust the health and medical experts they engage with personally, Ratzan says. Those experts should use language that comforts people who test positive and emphasizes that there’s nothing shameful about catching a widely circulating, highly contagious virus, Ratzan says. Social media is a useful tool for widely distributing constructive messages, he adds. Over time, Venetis says, the way we talk about and perceive COVID-19 will likely shift on its own. The Omicron variant may have helped hasten this process, since it continues to infect even triple-vaccinated people who wear masks—driving home the message that getting sick is not a moral failing, but a practically unavoidable fact of life as we now know it. from https://ift.tt/j6A1zSw Check out https://takiaisfobia.blogspot.com/ Getting vaccinated and boosted dramatically increases the likelihood of surviving a case of COVID-19, but many risk factors—like being biologically male—are outside of people’s control. In the U.S., 20% more men have died from COVID-19 than women, according to data from the U.S. Centers for Disease Control and Prevention. Scientists theorize that the difference in risk between the two sexes may, in part, come down to the hormone estrogen, which plays a role in the immune system. New research published in BMJ Open on Feb. 14 links estrogen levels to women’s likelihood of dying after they contract COVID-19. In the study, researchers looked at Swedish national health registry data from more than 16,000 women, ages 50 to 80, who had tested positive for COVID-19 between Feb. 4 and Sept. 14 of 2020. Most had gone through menopause, a time during which estrogen typically drops. Researchers were particularly interested in the women in the group who were taking medications that affect estrogen levels: 227 were on endocrine therapy, a treatment for breast cancer that lowers estrogen, and about 2,500 were undergoing hormone replacement therapy, which increases estrogen levels in order to reduce menopausal symptoms. After researchers factored in the women’s comorbidities, age, and socio-economic factors, they found that women who were taking medications that raised estrogen levels were about half as likely to die from COVID-19 as women who weren’t taking medications that affect estrogen. (There was also an initial link between taking estrogen-lowering medications and having an increased risk of dying from COVID-19, but after factoring in the confounding variables, it was not significant.) The finding fits with those from other observational studies that have also linked high estrogen levels to a lower risk of becoming seriously ill from COVID-19, says Dr. Franck Mauvais-Jarvis, director of the Sex-Based Medicine Laboratory at Tulane University (who was not involved in the study). Estrogen—and the hormone progesterone, to a lesser extent—is believed to be involved in the body’s immune response and may limit inflammation, he says. In COVID-19, inflammation can trigger a “cytokine storm,” a dangerous condition in which the immune system can get overwhelmed. Read More: To Ease Menopause Symptoms, Add a Little Melody Other research suggests that estrogen may also affect spike protein receptors, which SARS-CoV-2—the virus that causes COVID-19—uses to get into cells, says Dr. Malin Sund, a professor at Umeå University in Sweden and co-author of the new study. However, as Sund and her fellow authors point out, randomized clinical trials are necessary to determine whether the link is causal, and if artificially increasing estrogen can protect patients from COVID-19. The new study is not without drawbacks; for instance, the researchers were unable to check the women’s hormone levels over time. Sund emphasizes that people should not experiment with altering their estrogen levels; raising estrogen levels can have side effects, such as an increased risk of breast cancer. Conversely, “women who have had breast cancer should absolutely not stop taking their endocrine therapy based on this study because they really need their treatment for breast cancer,” says Sund. “The best thing they can do is get vaccinated.” Many diseases affect men and women differently, but throughout much of history, scientific research has focused on males alone. The U.S. National Institutes of Health didn’t make it an official policy to include women in clinical trials until 1989, and it didn’t require grant applicants to balance sex in research on cells and animals until 2014. Studying sex differences and disease shouldn’t stop with COVID-19, Mauvais-Jarvis says. “There are a lot of diseases—not just COVID-19—that are characterized by differences between men and women,” he says. from https://ift.tt/fqMile2 Check out https://takiaisfobia.blogspot.com/ SACRAMENTO, Calif. — California became the first state to formally shift to an “endemic” approach to the coronavirus with Gov. Gavin Newsom’s announcement Thursday of a plan that emphasizes prevention and quick reaction to outbreaks over mandated masking and business shutdowns. The milestone, nearly two years in the making, envisions a return to a more normal existence with the help of a variety of initiatives and billions in new spending to more quickly spot surges or variants, add health care workers, stockpile tests, and push back against false claims and other misinformation. “We are moving past the crisis phase into a phase where we will work to live with this virus,” he said during a news conference from a state warehouse brimming with pandemic supplies in Fontana, east of Los Angeles. The first-term Democrat, who last year survived a recall election driven by critics of his governance during the pandemic, promised the state’s nearly 40 million residents that as the omicron surge fades, “we’re going to keep them safe and we’re going to stay on top of this.” A disease reaches the endemic stage when the virus still exists in a community but becomes manageable as immunity builds. But there will be no definitive turn of the switch, the Democratic governor said, unlike the case with Wednesday’s lifting of the state’s indoor masking requirements or an announcement coming Feb. 28 of when precisely schoolchildren can stop wearing face coverings. And there will be no immediate lifting of the dozens of remaining executive emergency orders that have helped run the state since Newsom imposed the nation’s first statewide stay-home order in March 2020. “This pandemic won’t have a defined end. There’s no finish line,” Newsom said. The World Health Organization declared the COVID-19 outbreak a pandemic on March 11, 2020, and with omicron fading in many parts of the world some countries have begun planning for the endemic stage. But no state has taken the step Newsom did and offered a detailed forward-looking plan. Republicans have been frequent critics of Newsom’s handling of the coronavirus and were quick to disparage his latest effort. State GOP Chairwoman Jessica Millan Patterson called it “an extra-large helping of word salad” and renewed the call to “follow the lead of other blue states and end his state of emergency or lift his school mask mandate.” Newsom’s plan sets specific goals, such as stockpiling 75 million masks, establishing the infrastructure to provide up to 200,000 vaccinations and 500,000 tests a day in the event of an outbreak, and adding 3,000 medical workers within three weeks in surge areas. Newsom’s administration came up with a shorthand acronym to capsulize key elements of its new approach: SMARTER. The letters stand for Shots, Masks, Awareness, Readiness, Testing, Education and Rx, a reference to improving treatments for COVID-19. Dr. Jeffrey Klausner, an epidemiologist at the University of Southern California, said while some may argue these should have come sooner, he believes “the timing is right on.” “Surveillance, testing, vaccination, and treatment make the context very different and make it appropriate to shift our response from a pandemic response of trying to do everything possible, to a more rational response to try to implement things that we have strong evidence that work,” Klausner said. The plan includes increased monitoring of virus remnants in wastewater to watch for the first signs of a surge. Masks won’t be required but will be encouraged in many settings. If a higher level of the virus is detected, health officials will determine if it is a new variant. If so, state and federal officials have a goal to within 30 days determine if it responds to existing tests, treatments and immunities from vaccines or prior infections. California’s health secretary, Dr. Mark Ghaly, said one of the goals is to avoid business closures and other far-reaching mandates. However, he said the state’s requirement that schoolchildren be vaccinated against coronavirus by fall remains in effect. The plan includes new education, including “myth-buster videos” to fight misinformation and disinformation and help interpret ever-evolving precautions for a confused public whiplashed by safeguards that seemingly shift by the day and vary across county lines. In coordination with the federal government, it calls for a first-in-the-nation study of the pandemic’s direct and indirect impacts long-term on both people and communities. All this will cost billions, much of it already outlined in the pandemic response package Newsom sought as part of his budget last month. That includes $1.9 million that lawmakers already approved to boost staffing at hospitals and increase coronavirus testing and vaccine distribution, as well as existing money and anticipated federal funds. His proposed budget also includes $1.7 billion to beef up the state’s health care workforce, with more investment in increased laboratory testing capacity, data collection and outbreak investigation. Newsom, who has faced criticism for sometimes failing to follow his own rules, defended keeping in place some of his executive emergency orders, which he said most recently have allowed the state to quickly bring in temporary medical workers and to quickly distribute more than 13 million home test kits to schools. Those orders have dwindled from 561 to fewer than 100 in recent months, he said, and his administration is working with legislative leaders to eventually make them unnecessary. from https://ift.tt/1fcbGtX Check out https://takiaisfobia.blogspot.com/ Americans Are Still Living With a 2020 Attitude Toward COVID-19 Risk. Its Time for That to Change2/17/2022 As the pandemic has evolved and most Americans have sought vaccines for protection, and as those who chose to forgo vaccination became infected (often more than once), the risk that COVID-19 poses for most Americans has declined. It’s estimated that more than 90% of Americans have some level of immunity to COVID-19 through vaccination or prior infection. Along with this wall of immunity, approaches adopted when we had few tools to prevent spread are no longer providing benefits that always justify their costs of social disruption, diminished classroom experiences, and economic drag. But we’ve been slow to adapt our strategies to the evolving notions of risk. The CDC is soon expected to update its policies, moving away from national recommendations and instead tying to measures of local prevalence its guidance for the protective steps people should take. This community-by-community standard may not be enough. We’ve turned restrictions on but haven’t turned them off as conditions changed. In many cases, it’s because we’re still relying on the same metrics that we used at the start of the pandemic. These concepts for measuring risk have remained mostly fixed since that time, even as people acquired protections from the virus. [time-brightcove not-tgx=”true”] At the outset of the pandemic, we had a shared sense of the threat and a shared willingness to sacrifice a lot to deal with it. As the pandemic has evolved, and its burdens accumulated, that social compact has frayed. Now we need to shift from measures adopted collectively, to tactics taken individually by people who are judging their own individual risk against their degree of caution. This means we must accept more regional and local variation in measures adopted at the state level. The government’s role will be to make sure people have the tools they need to make those choices. Steps that were critical in 2020 to reduce death and health care strain when we were overwhelmed are no longer justifiable. But what anchors that change? Even when actions were adjusted based on risk, in many cases it came too slow. Without deliberate guideposts, it’s hard to gauge why one posture should give way to another, and how to make these decisions. We’ll never go back to many of the tragic steps we had to take in the spring of 2020 when we were overwhelmed by the first wave of the virus. Take the 45 days to slow the spread put in place by President Donald Trump to try and mitigate that devastating first wave. Reflecting on those extreme measures, it’s hard today to remember how bad it was back then because we haven’t anchored the debate in a consistent measure of danger and recovery. The New York City healthcare system had all but collapsed. We used hospital ships and triage tents pitched in Central Park to try and manage a devastating cascade of disease and death. The White House rightly judged that if other American cities fell, the nation would be overwhelmed. At the time, one White House official told me that in such a circumstance, the federal government would be tapped out, and wouldn’t be able to give another city the “New York treatment.” It was a reference to the extraordinary support that New York received. The comment stuck with me. Read More: The Omicron Wave Is Receding But the Pandemic Is Far From Over Remember that the CDC had failed to field a diagnostic test that could tell us where COVID-19 was spreading, and where it hadn’t yet arrived, so we couldn’t target our steps to the cities where the virus was already epidemic. We didn’t know where COVID-19 was, or where it wasn’t. We badly misjudged the scope of the seeding that was underway in cities like New York and Seattle. People were still arguing that COVID-19 was no worse than the flu, with a case fatality rate of 0.1 percent. By July 2020, when that first wave had subsided, 0.25 percent of the entire population of New York City had died from COVID-19, but only one-fifth of the City’s residents had been infected. The risk from COVID-19’s continued march was a catastrophic prospect. Our tools to limit its spread didn’t exist. And our vulnerability seemed unbounded. We had no immunity. We had no effective medicines. We didn’t know how to properly care for the patients admitted to our ICUs. We had to slow the spread and buy ourselves some time to get our response in place. At the epidemic’s peak during the winter of 2020, more than 6,000 people in the U.S. were dying each week in nursing homes alone. That was 2020. Now in 2022, we need to leave those 2020 notions of risk behind. What was judged to be “moderate” prevalence this time last year, when we were largely unvaccinated, may be the new “low” when our vulnerability has declined. Especially as we confront a more transmissible but less severe strain like Omicron. Since then, more Americans have acquired immunity through vaccination and successive waves of infection. By some estimates, almost 70% of Americans have been infected at least once. About 87% of adults have had at least one dose of vaccine. We have a growing reserve of therapies that can treat the sick and substantially reduce the risk of hospitalization or death. The U.S. will soon be producing almost a half-billion “at-home” COVID tests each month. We’ve also seen dramatic advances in our care of the sick. Yet a lot of the other constructs have stayed in place, even as the Omicron wave has started to subside. Until very recently, many children were still wearing masks in schools, with no agreed-upon standard for when that will end. When Omicron peaked, some schools reverted to remote learning. Offices are closed in many big cities. Some states and businesses are still mandating vaccines, trying to coerce a shrinking pool of vaccine holdouts at the cost of increasing acrimony, even as many of the unvaccinated have probably been infected, some more than once. Read More: Why COVID-19 Case Counts Don’t Mean What They Used To Confidence in public health has eroded because we’ve been too slow to adapt the steps we take to changing notions of risk. Some people are adopting their own measures to reduce their risk and voluntarily choosing to avoid congregate settings, wear masks, and take other precautions. Many people are excessively vulnerable to COVID-19 because of age or health conditions, and those who remain worried should have access to tools and support to keep safe. There’s understandable apprehension among parents torn between fears of the virus and the steps to keep kids safe, especially toddlers. But for those who feel more confident about the declining risks, we can only ask so much of the public for so long. There is an amassed effect from the disruptions. People are exhausted. Livelihoods and people’s mental health have been hurt by the diminished lives we’ve had to compromise around. Many children haven’t known a normal school day for two years. The constant disruptions take a cumulative toll. We never agreed that the costs can outweigh the benefits. The problem is we have no way of measuring these trade-offs, and no framework for deciding when to turn things on and, equally important, turn them off. Take the debate over pandemic and endemic. There’s no clear nomenclature for what it will mean when the virus becomes a persistent but manageable risk that doesn’t dominate our lives. Public-health leaders have different definitions of what it means when the pandemic gives way to an endemic state, where COVID-19 is part of the predictable repertoire of circulating pathogens. The simplest way to define that transition is when constant waves of excessive infection no longer plague the country, and COVID-19 settles into a more predictable pattern that follows the seasons. Some, including me, think that 2022 will be the year that we make this transition. Others still rate as high the risk that another unexpected variant emerges and wrecks that forecast. Regardless, it will remain an ongoing and persistent risk and will require us to be more vigilant around respiratory diseases, especially in the wintertime when these pathogens are most prone to circulate. We’ll need to protect settings where vulnerable people congregate and create incentives for people to stay current with vaccines. We’ll need to improve air quality and filtration in indoor settings. We’ll need to ensure widespread access to testing and create new cultural norms around staying home from work or school when you don’t feel well. We should distribute home diagnostic tests widely so consumers have a small stockpile on hand at all times. Masks could be used on a voluntary basis and become a tool for certain settings and for brief periods, to deal with epidemic peaks. We also must continue to innovate, investing in therapeutics that can treat the sick and provide for their wide distribution. But so long as we remain mired in a 2020 doctrine for measuring prevalence and how it correlates with risk, we’re going to be unable to adapt public-health measures to the virus’s ebb and flow, or find a common touchstone for managing risk in our lives. COVID-19 will remain a fearsome virus for the foreseeable future, but one that we must learn how to live with. Federal health officials have steered us through one of the hardest periods in our country’s modern history, and helped preserve life, even as we lost more than 900,000 of our fellow citizens. We’ve gradually found a way to coexist with this virus. Now we need a glide path to what normal becomes and a new math to guide how we adapt to COVID-19 even if we never fully defeat it. from https://ift.tt/ApfhTcx Check out https://takiaisfobia.blogspot.com/ To access the main road from his home high in the Himalayan mountains of the Indian state of Uttarakhand, Ram had to first climb down a mile of steep, unpaved, sloping path. From there, it was another 90 minutes on the main road to the village of Padampuri. That’s where the only government hospital and walk-in COVID-19 vaccination center in the Dhari area—home to some 30,000 people spread across 46 villages—is located. It was early September, and India was still recovering from a devastating second COVID-19 wave, driven primarily by the Delta variant. According to official government figures, more than 400,000 Indians died between June 1, 2020, and July 1, 2021, but a recent report in the journal Science estimated that the true toll might have been as high as 3.2 million deaths. The majority of those—2.7 million—occurred in three months, April through June 2021. [time-brightcove not-tgx=”true”] 
In the following months, cases of COVID-19 dropped significantly, and hospitalizations remained relatively low even during an Omicron-driven third wave, which peaked in late January. This is in part thanks to nationwide efforts to stop the virus. India began rolling out COVID-19 vaccines in January 2021, starting with health workers, then for people over 50 and those with comorbidities. It took a while for the vaccine rollout to pick up pace, but by Jan. 30 of this year, India’s government said 75% of its adult population had received two doses of a COVID-19 vaccine. Read More: How Did India’s COVID-19 Crisis Become a Catastrophe? As a septuagenarian, Ram was eligible early on, but at first he stayed home. He’d been unwell and felt uncertain about the safety of the vaccines. He was also wary of the trip he’d have to take to get his shots. But months of persistence by the health workers in Padampuri—and especially by his daughter-in-law, who is part of Dhari’s vaccination team—managed to persuade him. “I saw how hard she worked on this,” Ram says. “She urged me to take the vaccine, if not for myself, then for my family and the community.” His change of heart wasn’t unusual. Despite early concerns, in this isolated region that spans more than 30 sq. mi.—most of it rugged terrain that rises to 7,000 ft. of elevation—by the beginning of October, 100% of eligible adults had received a first dose of a COVID-19 vaccine. That equates to some 28,000 people, according to Himanshu Kandpal, the chief medical officer of the Dhari area, who is in charge of Padampuri’s medical center. The state of Uttarakhand as a whole reached that same milestone in mid-October, with all eligible adults—some 7.4 million people—receiving a first dose, usually of the Oxford-AstraZeneca vaccine, known locally as Covishield. (Those vaccinated in the very first phase typically received Covaxin, India’s own vaccine.) While most Indian cities are now catching up, Dhari was an early success story, and continues to get people to show up—more recently, for their second doses and booster shots. As of the time of writing, over 80% of eligible adults in Dhari, one of the most remote places in the world, have received a second dose, despite heavy snowfall and road closures in hilly areas. Kandpal says that by the end of February, the adult population in the region will be fully vaccinated—though it’s difficult to be completely certain in a region where officials struggle to document the members of every household. All eligible teenagers of ages 15 to 17 have also received a first dose. Other districts in the state have had similar success, as has India’s northernmost mountainous state of Himachal Pradesh. Indeed, the vaccination rate in Dhari and other hill districts far outstrips those of much richer places with better health infrastructure and where vaccines are widely and easily available. In the U.S., for example, 64.4% of adults have been fully vaccinated as of Feb. 14, while 75.9% have had a first dose. How did a remote Himalayan region manage to succeed where so many other cities and countries have struggled? The answer underscores the value of health workers who are embedded in their communities and know how best to serve them in a crisis. 
At first glance, Dhari seems an unlikely place to hit such a vaccine-success milestone. For one thing, the Indian government made a smartphone app the primary means for booking a vaccination appointment—in a country where only around half of the population has a smartphone. In rural areas like Dhari, that proportion is far lower. Another challenge was simple practicality. “Much of the population here lives in remote areas, and it takes them so long to come to the medical center,” Kandpal told TIME in August, sitting in his office in Padampuri—the only significant medical facility for 25 miles. The building, covered in faded yellow paint, stands atop a mountain slope, approachable only by a long flight of steep stairs carved out of the mountainside. At about 5,200 ft. of elevation, it is thousands of feet below many of the mountain villages it serves. “People have to commit to a full day to get vaccinated. That didn’t help,” Kandpal said. Hema Devi knows just how difficult that can be. In July, the 45-year-old farmer made the steep mile-long uphill trek from her home in the remote hamlet of Thiroli, to a vaccination camp in the bigger village of Dhanachuli. She waited for hours for her turn, before learning that the camp had just run out of vaccines. “I hear about people not taking the vaccines in the cities, and I am puzzled,” she says. “They don’t even have to climb a mountain or negotiate broken roads. They also don’t have to think of who’s going to cook dinner or lunch if they are stuck at the camp—they can just order food on the phone.” On Aug. 2, she tried again, waking before dawn to cook, clean, and take her buffaloes and goats out to graze before setting off with her husband and two neighbors. When they arrived in Dhanachuli, Devi and her husband joined different lines to register for their shots. The line for men was much shorter, with most of them—including Devi’s husband—there to receive second doses, while most of the women had yet to receive their first. That disparity has persisted across India, in part because of the difficulty in getting time away from housework and childcare. According to India’s official vaccination website CoWIN, as of Feb. 14, a total of 1.67 billion vaccine doses have been administered in India: 49.5% to women and 50.5% to men—a gap of some 38 million doses. Indeed, when Devi’s husband received his first dose in July at the primary health care center in Padampuri around an hour’s drive away, she couldn’t go with him because of home responsibilities. “It would have taken the whole day, and who would have taken care of the children and the housework?” Even on the day Devi finally received her vaccine, she rushed home after registering at the camp, to cook lunch and tend to the livestock while her husband saved her spot. She sprinted back just in time for her shot. “I didn’t want to miss out this time too,” she says. “If we run out of vaccines, you never know when we will get it next.” 
Devi wasn’t always so eager to get the vaccine. Like many Dhari residents interviewed by TIME, she was initially scared. “We heard stories of infertility and deaths,” she says. “But then we saw people taking it and they were OK. Also the health workers came to the village and explained and encouraged us. They are one of us, so we trust them.” Crucially, these workers have history on their side. The health care workers in Dhari are mostly local women who have been trained to act as educators in their communities through work as accredited social health activists (ASHAs) or hired by the government as nurse-midwives (ANMs) to act as the first point of contact between the community and the public health care system. Across India, especially in rural areas, these community workers have played a crucial role in the pandemic, creating awareness about the virus, tracking and monitoring cases, and then rolling out the vaccination program. In Dhari, this well-earned trust led locals to buy into the idea that they needed to get vaccinated to protect themselves and their families against COVID-19—even if it meant trekking hours through steep terrain. The success of Dhari’s COVID-19 vaccination campaign was also built on years of outreach within remote communities, especially among women and children, notably through India’s robust universal immunization program that reaches around 26.7 million newborns and 29 million pregnant women each year. That program relies on a broad network of district hospitals, primary health centers, government health workers, and community volunteers. It’s also credited with the country’s incredibly successful polio-vaccination campaign, which began in 1994, when India accounted for around 60% of global polio cases. Millions of frontline workers took on the task of vaccinating 170 million children under 5, twice a year. In 2014, two decades after the campaign began, India was declared polio-free. India’s immunization program for children may be “a well-oiled machine,” says Rajib Dasgupta, who heads the community health program at Jawaharlal Nehru University, but the system still needed to be adapted to deploy COVID-19 vaccines to adults. Kandpal and his team of 13 ANMs and 46 ASHAs consulted with village heads across Dhari to tweak the existing immunizing infrastructure to address the practical issues around travel and the lack of smartphones. First—and long before most areas in India began doing so—they decided to send out mobile teams to villages because not enough people were coming down to the two walk-in centers. While the polio-vaccine program includes a follow-up door-to-door campaign, this was a significant scaling-up to cover the entire adult population. These new mobile teams were capable of trekking into the mountains to get closer to isolated communities, where they established pop-up vaccination sites designed to get more shots into arms—both for those people who already want it and those who aren’t so sure. Read More: How the Pandemic Is Reshaping India Kandpal’s team also added fully equipped ambulances to the mobile teams in case of adverse reactions to the vaccines, a data-entry operator to register the villagers on the government vaccine app, and a pharmacist to hand out acetaminophen and advise people on what to expect after their shots. Kandpal also set up a WhatsApp group between local health workers and the village heads, posting the weekly vaccination schedule so that village heads could communicate with villagers. “COVID taught us to think out of the box. The systems it forced us to create will go a long way in the future too, to cater to this population,” Kandpal says. “We have taken an existing but old resource and modernized it.” 
On Sept. 4, nurse-midwife Renu Sharma—a member of Kandpal’s team who has been working with the Dhari population for 13 years now—traveled with a team of health care workers from Padampuri to the remote village of Aghariya. There, she received a warm welcome. She knew lots of the women by name, having vaccinated their children years earlier, and in a mock-stern voice, she told them to come and get their own COVID-19 vaccines at the camp now. Before the arrival of Sharma and her team, the nearest place for Aghariya residents to get vaccinated was the camp in Dhanachuli—a tough journey along an unpaved path that could be particularly treacherous whenever rains loosened the rocks and soil. That’s why Sharma and her team decided to set up a temporary pop-up vaccination site in Aghariya. They were quickly inundated, and by the afternoon the line for vaccines continued to grow. While administering shots, Sharma noticed a group of three elderly men who had spent the day sitting at the pop-up vaccination clinic. During a lull in activity, she approached them. “Bubbo, have you registered?” she asked, using a local term of respect meaning grandfather. They demurred. “No, no, we came here just to see what’s happening,” one said. “We don’t want to take the vaccine.” Undeterred, Sharma continued to press: “Look at me, bubbo, I was one of the first ones to take the vaccine. Has anything happened to me?” she said. At that point, others in the village who had gotten a shot joined in, saying they too had suffered no serious side effects. Finally, the men relented. Sharma marched them to the registration table with a triumphant smile and went back to her station to open up another pack of the vaccines. “Sometimes you have to persist with them a bit,” she said. “I have had to persist for days and weeks with some people.” 
At the end of the day, Sharma consulted her list of village residents and checked them against those who had registered to be vaccinated. She found the names of three elderly and disabled people with mobility issues who she knew couldn’t make it to the camp. She took a bag with vaccine doses and supplies and walked with her team toward their homes, a short trek from the vaccination site. An official door-to-door vaccination policy would only be announced by Prime Minister Narendra Modi in another two months, but Sharma’s prior work had taught her that sometimes you need to meet people where they are. Health workers like Sharma know well the challenges in the smaller communities they serve, whether travel difficulties or household commitments—a kind of knowledge and intimacy that is impossible in bigger cities. At the Aghariya camp, she did not waste an opportunity to advise mothers who were there for routine immunizations for their kids that they should also get the COVID-19 vaccine for themselves. “You have to be mindful of the community’s sentiments,” she says. “We don’t push too hard. It takes time. Sometimes I request, sometimes I am stern. But they know I mean well.” Throughout the last months of 2021, Sharma and others like her worked unremittingly to get vaccines to people in remote villages. Hema Devi, who got her first shot in August, was able to get her second in December—though she still had to make the long trek from Thiroli to Dhanachuli. She was relieved to get it when she did, as an Omicron-fueled surge of COVID-19 cases began sweeping the country shortly after. Several weeks later, India’s COVID-19 cases are on the decline, and state governments are reopening schools after long hiatuses. In Dhari, where cases are also falling and hospitalizations remain relatively low, health workers are still working to fully vaccinate 15- to 17-year-olds, as well as administer booster shots to adults. Though cases are now falling and hospitalizations have remained relatively low, health workers in Dhari are still working to fully vaccinate 15- to 17-year-olds, as well as administer booster shots to adults. Sharma says it’s much easier this time than with first doses because there’s a much greater understanding of the need for them. Villagers have “watched the news about the booster dose on television and have been coming up to me asking about it,” she says. “They understand the importance of the vaccines in keeping the whole community safe.” That understanding helps people like Devi to walk the extra mile to get vaccinated. “If I could, I would urge everyone to take the vaccine. Don’t think of yourself; think of your friends and family and your community,” she says. “If you are safe, they are safe; the world is safe.” --With reporting by Eloise Barry/London from https://ift.tt/8eyISCb Check out https://takiaisfobia.blogspot.com/ Pediatricians Who Serve Trans Youth Face Increasing Harassment. Lifesaving Care Could Be on the Line2/16/2022 Dr. Gina Sequeira first saw the protesters on a bright clear morning last September. A co-director of Seattle Children’s Gender Clinic who provides gender-affirming care to young people, Sequeira had confronted ignorance about her medical specialty in the past. But nothing had prepared her to see people outside her office, waving signs and handing out flyers warning of the “dangers” of the work she does. “That was really, really hard for us as a clinic,” she says. “And I think it was really hard for the hospital’s patients and families who witnessed it.” Just a month later, protesters showed up again. Hers wasn’t the only clinic having a hard time in 2021. The LGBTQ advocacy group Human Rights Campaign has calculated that, last year, conservative lawmakers introduced over 130 anti-trans bills into state legislatures--including 35 that explicitly limited the ability of trans and gender-expansive youth to access gender-affirming care, a term that refers to holistic psychological and medical care that affirms a person’s gender identity. As of Feb. 11, the ACLU has tracked similar bills in at least 17 state legislatures this year. Only a small group of pediatricians provide such care in the U.S., and, in this political context, those who do are often finding themselves at the receiving end of growing harassment—even as research confirms the potentially life-saving nature of the work they do. Demonstrators have organized protests like the ones at Sequeira’s clinic at other sites across the country; in Ohio, billboards have been rented spreading disinformation about affirming care—including one near a children’s hospital. Pediatricians tell TIME they have received threatening mail, have been impersonated online and have feared for their safety. And they worry such harassment campaigns could have a devastating impact on the ability of young people to access crucial medical care. Roughly a month before the September protest, Sequeira had received an unmarked letter in the mail that gave her pause. She’d worried about the risk of anthrax, she tells TIME; of someone trying to hurt her. Eventually she gingerly opened the envelope. Inside, she found printed posters decrying gender-affirming care for children. “No child is born in the wrong body!” one read. “Who profits from this crime?” “I was taken aback, and really kind of fearful,” Sequeira recalls. She’d seen colleagues who provided abortion receive similar abuse. But she never thought her work could become nearly as controversial. “It really made me wonder what the future of our work looks like,” she says. “Is that the path we’re going down?” 
Gender-affirming care can support youth experiencing gender dysphoria, which is often described as the discomfort or distress that might occur when a person’s gender identity is inconsistent with the sex they were assigned at birth, per the Mayo Clinic. In gender-affirming care models, according to the American Academy of Pediatrics (AAP), “pediatric providers offer developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience.” That includes conveying the message that variations in gender identity and expression are a normal aspect of human diversity, and that, if a mental health issue does exist, it “most often stems from stigma and negative experiences rather than being intrinsic to the child.” In young children, gender dysphoria can be treated with non-medical social and behavioral interventions, which can include allowing a child to present themselves in alignment with their gender identity by changing the way they dress, for example, or changing their given name and pronouns, explains Dr. Morissa Ladinsky, a pediatrician at the University of Alabama at Birmingham who specializes in affirming care. Read more: Gender-Affirming Hormone Therapy for LGBTQ Youth Can Help Save Lives, Study Finds After puberty has begun, a child experiencing gender dysphoria may also begin receiving gonadotropin-releasing hormone (GnRH) analogues—known by the term “puberty blockers.” They are “simply a pause button,” says Ladinsky, to stop the continued development of a puberty incongruent with a child’s gender identity. Used at this stage, blockers are reversible, says Ladinsky, and have been used safely for over 30 years in other pediatric conditions like central precocious puberty, which causes children to enter the developmental stage too early. Puberty blockers can help “reduce distress that may occur with the development of secondary sexual characteristics” and reduce the need for surgery in the future by holding off physical changes like an Adams apple or breast growth, according to the AAP. When they get older, some adolescents will begin taking gender-affirming hormones, such as testosterone or estradiol. While there is some debate within the medical community on when any given young person should start hormones, the intervention has proven pivotal to the treatment of dysphoria in many adolescents. It is rare for a person under 18 to undergo any type of surgical intervention, but some may decide to pursue “top surgery”—reconstructive surgery to change the appearance of one’s chest—while they are still teenagers. An emerging body of research has found that affirming care models can result in young people having fewer mental health concerns. As with all medical care, treatment decisions are nuanced, and, because of the age of the patients, are driven by conversations between the young person, their family and their doctor. Trans and gender expansive children cannot receive affirming medical treatment without their parent’s or guardian’s consent in the U.S. healthcare system. Yet much of the criticism surrounding gender-affirming care operates from the misperception that young children are receiving rushed, unsupervised, irreversible treatments. In violent, visceral terms, best-selling authors, right-wing commentators, conservative social-media stars, and other influential figures have made such arguments, stirring a moral panic that has grown in recent years. The Williams Institute at UCLA estimated in April 2021 that 45,100 trans youth were at risk of losing medical care if all the bills then under consideration that intended to restrict or ban gender-affirming care were implemented into law. In the same month, Arkansas went so far as to ban pediatricians from not only providing gender-affirming care, but even providing a referral to patients. (The law is currently blocked by a federal judge.) In August, Texas Gov. Greg Abbott suggested that providing affirming care to adolescents equates to child abuse. Mis- and disinformation about trans people has also gained airtime in conservative media, especially online. A Nov. 9 report from Media Matters found that 77% of the top-performing trans-related Facebook posts between Oct. 2020 and Sept. 2021 were on right-leaning pages, as were nearly two-thirds of all the interactions on posts about trans issues. “There’s nothing grassroots about this at all,” argues Imara Jones, journalist and founder of TransLash Media, whose podcast the Anti-Trans Hate Machine has documented the rapid rise of anti-trans legislation in recent years. “This is a highly organized movement that is targeting trans people and trans rights.”’ Jones traces the proliferation of anti-trans bills to an umbrella organization of over 60 right-wing groups called Promise to America’s Children, which lists on its website “leading national partners” including Family Policy Alliance (the lobbying arm of longtime anti-LGBTQ group Focus on the Family), Alliance Defending Freedom (which the Southern Poverty Law Center has defined as an anti-LGBTQ hate group), and conservative think tank The Heritage Foundation. She adds that the anti-LGBTQ group Family Research Council has actively promoted anti-trans bills. Promise to America’s Children’s website includes model legislation for policymakers titled the “Protecting Children from Experimentation Act,” which aims to criminalize gender-affirming treatment for young people. A version of the bill was introduced in Congress in 2021, though it did not advance. Leading medical organizations have decried such legislative bans. “[We] strongly oppose any effort to criminalize or penalize physicians for providing necessary care for their patients,” read a April 2021 joint press statement from AAP, the American Academy of Family Physicians, the American College of Physicians, the American College of Obstetricians and Gynecologists, the American Osteopathic Association, and the American Psychiatric Association. “Physicians must be able to practice medicine that is informed by their years of medical education, training, experience, and the available evidence, freely and without threat of punishment.” Read more: Anti-Trans Violence and Rhetoric Reached Record Highs Across America in 2021 This focus on gender-affirming pediatricians has extended beyond legislation. As disinformation and fearmongering about trans youth has surged, TIME has spoken with numerous providers who say they’ve witnessed a rise in harassment in the past two years—whether via in-person protests, online threats and cyberbullying, menacing mail, attempts to cut their research’s funding or even their medical licenses. Other gender-affirming pediatricians with whom TIME spoke refused entirely to go on the record, citing fears about the risk of violence against them and their families. “This is shocking, shocking, shocking,” says Dr. Robert Garofalo, the head of adolescent and young adult medicine at Lurie Children’s Hospital of Chicago. “No one is prepared for this, and pediatric institutions aren’t prepared for it.” 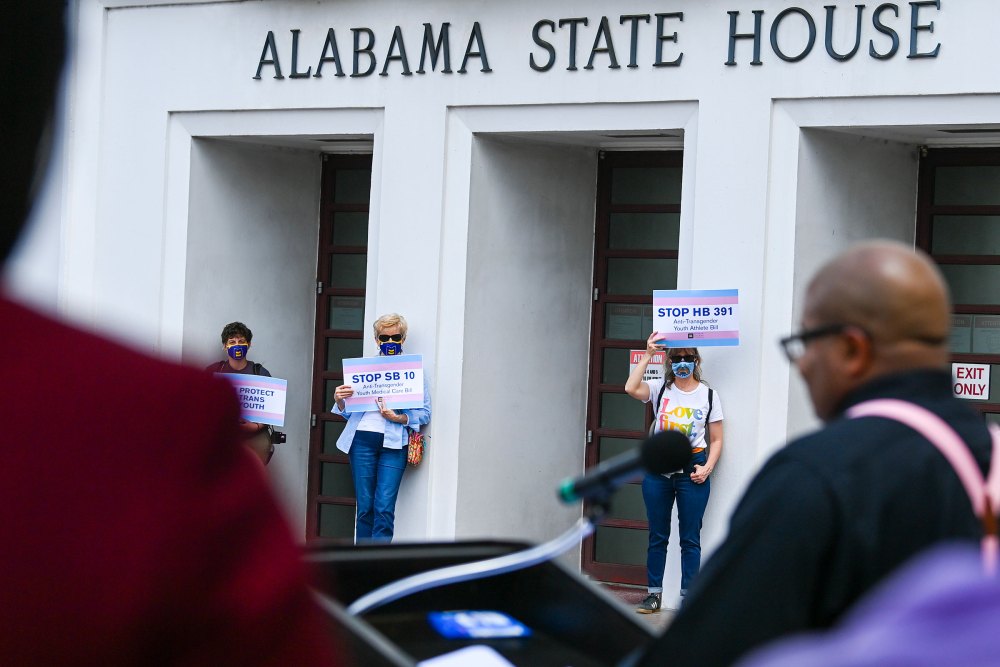
The first known protest of gender-affirming pediatricians was in December 2020, per research by Health Liberation Now (HLN), a trans-run advocacy website that researches political impacts on trans health. But by February of 2021, anti-trans groups had announced plans to protest in Los Angeles; Chicago; Philadelphia; Dallas; Hartford, Conn.; and Ontario, Canada. Through the summer and fall of 2021, protests became a more regular occurrence. Some anti-trans groups have begun using an online interactive map that tracks the location of clinics providing gender-affirming care, per HLN’s research. Other forms of harassment stay online, but pediatricians say they are similarly frightening—and have been going on since even before the first documented in-person protest. When Susan, a pediatric endocrinologist, got the call from her hospital’s administrative assistant in the fall of 2020, it felt like she’d been punched. (TIME is withholding Susan’s identity and that of one other provider out of concerns for their safety.) A patient’s family had contacted the hospital, the assistant said, flagging that they’d seen posts online from an account that was purporting to be Susan, but didn’t sound like her. Susan rushed to her computer, and sure enough, there was her picture and her name on a Facebook profile, apparently posting about how she regretted her treatment of transgender kids—a feeling that couldn’t be further from the truth. She found a similar fake account on YouTube pretending to be her, expressing “remorse” for her actions. At least three other gender-affirming pediatricians were impersonated in this incident, Susan tells TIME. Their posts were made to look as if they were in conversation with each other, agreeing about the “harm” they’d done to kids. “I don’t think I ever went into medicine thinking something like this could happen,” Susan says. “We’re always just trying to care for kids.” Things have gotten worse. In the spring of 2021, her clinic received threats about protests. In the fall of 2021, the protests actually happened. “It really made us evaluate our safety systems for our patients, families, and staff,” she says. Susan says that she’s repeatedly been threatened with being reported to her state’s medical licensing board—though her care is not in violation of any policies—and adds that she knows gender-affirming mental-health clinicians who have faced similar harassment. Leigh, a pediatric endocrinologist in the southeast, says people have tweeted at her asking her how she sleeps at night, arguing she is violating God’s plan. “I am here to take care of my patients and make sure that they live longer, better, healthier lives,” she says. “And to have someone suggest something otherwise is just devastating to me.” Late at night, she’s sometimes filled with a sense of dread over where this rise in harassment could be leading. “We’ve had active shooters in the hospital where I practice for years,” she says. What if one day one of those shooters came looking for her clinic, or even her private home? “That is one of my biggest fears.” Read more: America’s Foster Care System Is a Dangerous Place for Trans Teens. Now They’re Fighting for Change Garofalo, of Lurie Children’s Hospital, says that at least three of his colleagues in more conservative states reached out in 2021 asking for advice on how to deal with the harassment they were facing. They’ve told him “horror stories,” he says, including instances of receiving death threats. Dr. Brandon Hill, the former President and CEO of Planned Parenthood Great Plains, which operates in Kansas, Missouri, Oklahoma, and Arkansas, says he’s been contacted by children’s hospital administrators in major cities across the country asking what trainings he gives abortion providers to prepare them for intense backlash and harassment. “This stuff isn’t new. The tactics that these anti-trans-care folks are using have been used to [target abortion providers],” Hill explains. “[But] I don’t think we ever thought of this being something where protesters would be outside of adolescent health centers. Ever.” In response, many gender-affirming pediatricians have banded together to be each other’s support systems. “There are definitely colleagues who have to worry more about safety than others,” says Garofalo. “We check in on each other.” They hold wellness events and share experiences. “We’re trying to advocate and be united together,” Susan adds. “But I can see the potential for burnout.” 
The stakes couldn’t be higher. A peer-reviewed study published in the Journal of Adolescent Health on Dec. 14 found that the use of gender-affirming hormone therapy (GAHT) is significantly related to lower rates of depression, suicidal ideation, and suicide attempts among transgender and nonbinary youth. The study, led by researchers at the LGBTQ suicide prevention nonprofit The Trevor Project, also found that among young trans and nonbinary people under 18, receiving GAHT was associated with nearly 40% lower odds of having had a suicide attempt in the past year. Notably, half of the transgender and nonbinary youth surveyed said they were not receiving GAHT but wanted to. Several providers said they worry intimidation tactics could ultimately limit the health care options available to transgender and gender expansive youth, who already often face barriers to receiving care, including stigmatization, a lack of familial support, high costs, and onerous travel to reach clinics. “We don’t need another [hurdle],” says Sequeira. “We don’t need kids to have to walk through a gauntlet of protesters to get care.” Dr. Janet Cathey, a gender-affirming provider who treats adults and adolescents at the Planned Parenthood in Little Rock, Ark., also worries that primary care doctors considering offering gender-affirming care might choose otherwise because they don’t want to risk wading into controversial territory. In states such as Arkansas, where gender-affirming care for youth was temporarily banned in 2021, providers may feel nervous about treating trans youth because they worry it could threaten their medical license, she says. In a research study Sequeira has been conducting over the past year, several pediatricians expressed apprehension about starting to offer gender-affirming care, she says, in part because they feared for their safety. “Which is a shame, because we so desperately need more providers in this area,” Sequeira says. A lack of available doctors doesn’t mean young people will stop needing affirmative care, adds Susan. They might just seek that care in underground ways without the supervision of a doctor, which could be dangerous. Such an exodus has not occurred in the field of abortion providers, despite decades of dangerous attacks that include bombing, arson, and death threats, explains David S. Cohen, a professor of law at Drexel University and the author of Living in the Crosshairs: The Untold Stories of Anti-Abortion Terrorism. However, Cohen adds, many abortion clinics have been forced to close because of financial and regulatory restraints. If the trend of anti-trans legislation continues, the same could happen to gender-affirming care providers, whether or not doctors want to leave the specialty. “The impact of this harassment is broad. It affects clinical care. It affects research. It even affects philanthropic support, which for a lot of programs has been critical,” says Garofalo, who adds that there has already been “tremendous amount of efforts to defund” his research on gender-affirming care with the National Institute of Health. Read more: Andraya Yearwood, a Star of Hulu’s New Changing the Game Documentary, Talks Life as a Trans Athlete In November, the Children’s Medical Center Dallas and UT Southwestern Medical Center in Texas dissolved their six-year-old program that offered gender-affirming care to young people. (In a statement to the online news magazine LGBTQNation, the two medical centers said the decision to dissolve the program was the best option to maintain privacy for patients.) The decision came after organized protests that targeted hospital board members and argued that the care equated to child abuse, per the Texas Tribune. The program was the only one of its kind in the state. “That’s the part that really breaks my heart about all this,” says Sequeira. “There’s a lot that’s really challenging about being an adolescent, and especially an adolescent who is finding ways to affirm their gender.” “It just makes me so fearful to see the increasing number of protests and discrimination happening to us as providers,” she continues, “Knowing that, I can only imagine what’s happening in communities, for many, many kids.” —With reporting by Julia Zorthian from https://ift.tt/uHN7Qm6 Check out https://takiaisfobia.blogspot.com/ The latest revelations about Russian figure skater Kamila Valieva’s doping case raise more questions about the substances found in her sample—and the reasons why the 15-year-old might have failed the drug test. TIME asked leading experts to help make sense of the claims, which have upended the women’s figure skating competition at the Beijing Olympics and cast a larger pall over the sport. At the hearing held on Sunday by the Court of Arbitration for Sport (CAS), anti-doping authorities revealed that Valieva tested positive for three heart treatment drugs, one of which is banned as a performance-enhancer by the World Anti-Doping Agency. In addition to trimetazidine (TMZ), the prohibited substance, the New York Times reported that Valieva’s sample also contained hypoxen and L-carnatine, a supplement. All three are used for patients with angina, to improve blood flow and enhance function of the heart when it lacks oxygen. When she submitted a sample for testing in December, Valieva declared that she was taking hypoxen and L-carnatine, along with another compound, supradyn, a supplement that boosts immunity, according to documents reviewed by the Times. All three of those substances are allowed. To explain the presence of the prohibited drug, TMZ, Valieva’s lawyer argued that she was “contaminated” with the medication, potentially via contact with her grandfather, who appeared by video to say that he takes the medication. TMZ is prescribed to treat angina, because it can help increase blood flow to the heart and help the heart to work more efficiently. It’s not approved in the U.S., but is approved by the European Medicines Agency and other regulatory bodies. READ MORE: Kamila Valieva Is Allowed to Skate. The Battle Over Her Drug Test Is Just Beginning Russian newspaper Pravda reported that Valieva’s lawyers argued during the hearing, “There can be completely different ways how it got into her body. For example, grandfather drank something from a glass, salvia got in, this glass was somehow later used by an athlete. Or the drug lay down on some surface, traces remained, the drug lay down on this surface, which the athlete then drank.” Can the drug pass that easily from one person to another, and if so, would it appear in the recipient’s urine sample, as Valieva’s lawyer is claiming? “It reminds me of kids I knew who said they got venereal disease from the toilet seat,” says Dr. Steven Nissen, a cardiologist at the Cleveland Clinic. Nissen says he’s not familiar with how sensitive the assays, a scientific measurement procedure, being used by the WADA lab are, but says that testing positive for a substance by drinking from the same glass as someone taking it is “very far-fetched.” “It’s hard to be definitive without knowing the assay [test] sensitivity, but it seems very, very unlikely,” he says. Valieva’s lawyer also claimed she might have come into contact with the medication on a surface and then somehow ingested it. Dr. Donald Lloyd-Jones, president of the American Heart Association and chair of preventive medicine at Northwestern University’s Feinberg School of Medicine says, “I’ve seen no evidence it gets absorbed through the skin.” He admits he doesn’t know how much of the drug was detected in the athlete’s sample, which would inform whether a brief contact with a small amount of the drug could explain her positive test. Lloyd-Jones also points out patients have to take TMZ three times a day, because it is metabolized by the body and excreted relatively quickly. Taken at the approved dose, the drug would reach its peak levels in the blood in anywhere from two to six hours, and the majority would be cleared within 24 hours. “It would seem implausible that a little bit on a glass or on her skin would have resulted in a positive test unless it happened to be just before she provided the sample,” he says. “One can draw inferences that either the exposure was very recent, very shortly before her test, or that she was exposed more chronically.” Ideally, a performance-enhancing drug has the same feature. “The ideal performance-enhancing compounds get in to improve performance, then get out without leaving a trace,” says Lloyd-Jones. READ MORE: Olympians Let Loose on Kamila Valieva and Russian Doping Controversy While TMZ is not available in the U.S., Nissen says there is a similar drug, ranolazine, that is approved by the Food and Drug Administration. That drug also shifts the energy source that heart cells use from fatty acids to glucose, which is more efficient. “That’s why it works for angina,” says Nissen. “It allows people to do more with less blood flow. Conceivably for an athlete, it would have similar benefit and would make the heart work more efficiently and give them a little edge.” Lloyd-Jones says this metabolic pathway also results in less build-up of lactic acid, which can cause muscle fatigue. “There are data from small trials in patients who have heart failure that that seem to indicate better heart performance for those who have a failing pump,” he says. “But whether that translates into the same benefit in a young, healthy person—I don’t think we know.” It’s also unclear what the consequences are of taking these compounds while the body is younger. “It’s certainly concerning, especially in a young person whose body is still developing,” says Lloyd-Jones. “We really don’t understand the long term effects of changing someone’s physiology at this age.” While the Court of Arbitration for Sport determined Valieva could compete in Beijing, her doping violation case remains unresolved, pending further investigation. That means the gold she and her teammates won in the team event, and any medal she wins in the women’s event could potentially be stripped if anti-doping officials conclude she doped and competed with an unfair advantage. That will hinge on additional testing of a second sample, provided from the same urine as her first, that will be analyzed to confirm the positive results from the first sample. from https://ift.tt/RQsbnwo Check out https://takiaisfobia.blogspot.com/ COVID-19 vaccination during pregnancy provides strong protection for both mother and baby, new data from the U.S. Centers for Disease Control and Prevention (CDC) suggest. Babies born to mothers who received two mRNA vaccine doses during pregnancy were 61% less likely to be hospitalized with COVID-19 in their first six months of life, compared to babies born to women who were not vaccinated during pregnancy, according to the CDC’s new report. The CDC recommends COVID-19 vaccination for pregnant people, since they are at high risk for complications if they get infected during pregnancy. Vaccination is safe and effective for mother and baby, the agency says. In November, the American College of Obstetricians and Gynecologists also recommended boosters for all eligible pregnant people. The new study, published Feb. 15 in the CDC’s Morbidity and Mortality Weekly Report, offers the first real-world evidence that vaccination during pregnancy can also help keep infants safe from the virus. Disease-fighting antibodies generated by vaccination seem to pass from mother to baby in utero and offer protection against severe disease and hospitalization, the study’s authors write. “Today’s news is highly welcome, particularly in the backdrop of the recent increase in hospitalizations among very young children,” said Dr. Dana Meaney-Delman, chief of the CDC’s Infant Outcomes Monitoring Research and Prevention Branch, during a press briefing. “Unfortunately, vaccination of infants younger than six months old is not currently on the horizon, highlighting why vaccination during pregnancy is so important.” The CDC’s study was fairly small; researchers examined data from almost 400 infants younger than 6 months who were hospitalized across 17 states from July 2021 to January 2022. Roughly half of those infants were hospitalized with COVID-19. The other babies were hospitalized for other causes and served as a control group. Across both groups, the median age was two months. About 20% of the babies had at least one underlying medical condition, and about 20% were born premature. Among the infants hospitalized for COVID-19, 84% were born to mothers who were not vaccinated during pregnancy, the CDC found. Babies born to mothers who were vaccinated during pregnancy were 61% less likely to be hospitalized with COVID-19 than babies born to unvaccinated mothers. The timing of the vaccination seemed to matter, as well. Babies born to mothers who were vaccinated at least 21 weeks into their pregnancies were 80% less likely to be hospitalized with COVID-19 than those with unvaccinated moms; that number dropped to 32% for babies born to mothers who got their shots in the first 20 weeks. Nonetheless, the CDC has not recommended vaccination at any specific point in pregnancy. While getting vaccinated in later trimesters might confer more protection to the baby, pregnant people are susceptible to severe disease and pregnancy complications if they do get infected, which also makes it important to be protected as early as possible, Meaney-Delman said during the press briefing. Vaccination rates among pregnant people have lagged behind those of the general U.S. population. That’s likely a holdover from the early days of vaccine rollout, when little was known about how the shots affected pregnant people and fetuses. Vaccination rates have risen in recent months, following the release of strong data on the shots’ safety and efficacy, but “we still have a lot of work to do,” Meaney-Delman said The new data may help persuade expectant moms. Since children under five are not eligible to be vaccinated against COVID-19, the report offers reassuring data to new and expectant parents during an otherwise frustrating time. A U.S. Food and Drug Administration expert committee was scheduled to meet on Feb. 15 to discuss expanding authorization of Pfizer-BioNTech’s vaccine to children ages 6 months to 4 years, but that meeting was postponed while Pfizer gathers more data from its ongoing clinical trial. That means babies and toddlers may not be vaccinated for months to come. However, as the new data show, parents-to-be do have a way to protect their newborns and themselves: getting vaccinated during pregnancy. from https://ift.tt/xzbWYF3 Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
