
(TOKYO) — Loaves of bread have been taken off store shelves in Japan after the remains of “a small animal” believed to be a rat were found. Production of the bread was halted at a Tokyo factory, with 104,000 packages being recalled, according to Pasco Shikishima Corp. The company apologized and promised compensation. “We will do our utmost to strengthen our quality controls so that this will never happen again. We ask for your understanding and your cooperation,” it said in a statement this week. Japanese media reports said at least two people who bought the bread in Gunma Prefecture, northwest of Tokyo, complained to the company about finding a rodent in the bread. The bread had been sold in various areas, including Ibaraki, Niigata, Kanagawa, Fukushima, Aomori and Tokyo, according to Pasco. The company, based in Nagoya city, central Japan, also makes rolls, bagels and muffins. Japan boasts relatively high food safety standards. But the nation has been rocked by food woes recently, including 1,000 schoolchildren sickened by milk and two people who got sick after eating steak at a restaurant, both earlier this month. Widespread food poisoning from a health supplement product broke out in March and killed five people. from https://ift.tt/lSkNwX3 Check out https://takiaisfobia.blogspot.com/
0 Comments

If H5N1 turns into a full-blown pandemic, we are currently in chapter one. To prevent chapter two from becoming a reality, the most important tool in our arsenal will be widespread testing. Testing isn’t just about diagnosing people with the virus. Containing the spread of this highly pathogenic bird flu strain in cattle hinges on our ability to detect and track it. The H5N1 outbreak in dairy cows is widespread and spans multiple U.S. states. Although only one human infection with the virus has been documented, more infections are likely going undetected. Most importantly, unchecked transmission among cattle means the virus is increasingly bumping up against humans. Every human exposure, in turn, provides an opportunity for new mutations that could enable human-to-human transmission. [time-brightcove not-tgx=”true”]The U.S. Centers for Disease Control and Prevention (CDC) maintains that as of now, the risk to the general public from H5N1 remains low. And indeed, it is entirely possible H5N1 might never turn into a human pandemic. However, being wrong would be incredibly costly. We find ourselves in a situation reminiscent of early 2020, when the U.S. stood on the brink of the COVID-19 pandemic and hesitated to take decisive action, restricting testing to only those with epidemiological links to China. Scientists estimate that by early March 2020, less than 1% of SARS-CoV-2 infections in the U.S. were detected by testing. We effectively flew blind straight through chapters one and two of the COVID-19 pandemic. Today, genomic analyses tell us that bird flu had been circulating in dairy cows for at least four months before it was detected in March 2024. The delay was despite early warning signs of infections on dairy farms in February. The U.S. government cannot afford to repeat the mistakes made at the onset of the COVID-19 pandemic. Though the risk of an H5N1 pandemic may currently be low, the consequences of inaction could be catastrophic, and the benefits of proactive testing far outweigh the short-term costs. Read More: Why Experts Are Worried About Bird Flu in Cows Despite the high stakes, government action initially has been slow and uncoordinated. Until mid-April, testing was not only voluntary but restricted to symptomatic animals, with limits on the number of tests per farm. A complicating factor is that responsibility for outbreak control is divided between three federal agencies: the U.S. Department of Agriculture (USDA) for livestock, the U.S. Food and Drug Administration (FDA) for food safety, and the CDC for human health and surveillance. Yet by May, the CDC was aware of only about 30 people who had been tested for bird flu. The CDC has been monitoring data from emergency departments in areas where H5N1 has been found in cattle and has found nothing unusual so far. But if and when infected people show up at the ER, it will be way too late to contain the outbreak at its source. We must stop flying blind. Regular and widespread testing is our only way to detect H5N1 and stop the virus from spreading. The recent federal order requiring mandatory testing of dairy cows before they cross state lines is a step in the right direction. But we could be doing more: we should incentivize testing, rather than restricting it. A layered testing strategy that combines waste or wastewater surveillance on the farms, routine testing of pooled milk from the cows, and active surveillance testing of animals and humans—including those without symptoms—is our best hope of stopping the virus from spreading. The tools and infrastructure for such a testing regimen are already at our fingertips. During the pandemic, the U.S. government spent billions supporting testing and creating an extensive biosurveillance infrastructure. Influenza monitoring via wastewater surveillance has already shown increases in the H5 subtype—the viral group to which H5N1 belongs. In 2024, labs across the U.S. now have PCR machines sitting idle, waiting to be turned back on. And U.S. test manufacturers have efficient automated manufacturing lines capable of producing millions of rapid tests a day. Read More: Is It Safe to Eat Eggs and Chicken During the Bird Flu Outbreak? For animal testing, we should accelerate evaluations of both laboratory and point-of-need tests. Testing should include cows, but also pigs, which are known “mixing vessels” for viruses across host species. We should also evaluate different specimens like swabs and cow milk, including the pooling of samples to test more efficiently. If existing influenza A rapid tests could detect the virus from a drop of contaminated milk, it would be a game changer. Given the sky-high virus loads detected in milk from infected dairy cows, it is possible that a single drop could be enough. But if the tests need to be tweaked, the USDA and FDA should be funding studies to do so now. With H5N1 circulating in herds nationwide, we can quickly assess the effectiveness of these tests and refine our strategies accordingly. When it comes to human testing, it is laudable that the CDC is now engaging with test manufacturers to develop a widely available H5N1 test. In the meantime, existing authorized rapid tests for influenza A will likely detect H5N1. To confirm, the CDC, FDA, and the National Institute of Health’s Rapid Acceleration of Diagnostics (RADx) program should support evaluations that close that knowledge gap. If these broad influenza rapid tests detect H5N1, we could send any positive influenza A test to a lab for confirmation and evaluation of H5N1 or another virus. This surveillance testing algorithm, which leverages broad influenza tests for initial screening and reserves more specific H5N1 assays for confirmation, followed by rapid sequencing of positives, would allow us to allocate our public-health resources with maximum efficiency. The rapid turnaround times of point-of-need tests would enable infected people to immediately isolate themselves and get influenza antivirals, minimizing the risk of transmission. The federal government keeps the influenza antiviral Tamiflu as well as personal protective equipment (PPE) in its Strategic National Stockpile. To ensure that tests are similarly available, the government must send a clear demand signal to manufacturers, committing to purchase a substantial quantity of tests, just as they do for antivirals and PPE. This would give manufacturers the confidence needed to ramp up production and create a robust national stockpile. Congress should allocate funding to support these efforts, with the White House’s new Office of Pandemic Preparedness and Response coordinating a unified response across the CDC, USDA, and FDA. The government must also address the stigma associated with positive test results and provide financial aid and resources to help affected farmers and their workers. Many of the individuals working on dairy farms are undocumented, for example. The current administration should make assurances that offer protection to undocumented workers who agree to test as a part of public-health surveillance testing programs. Success in public-health prevention is difficult to spot, and success in preventing a pandemic can be misconstrued as a failure or a misappropriation of funds. It’s nearly impossible to recognize the absence of a pandemic that never happens, but would have if not for aggressive and early efforts. However, tracking detections and documenting actions taken will help. The cost of inaction far outweighs the cost of prevention. We risk losing all the lessons learned from COVID-19 if we don’t apply them now. The good news is that we have the tools to prevent an H5N1 pandemic at hand. But we must be willing to use them, and fast. from https://ift.tt/EkACxd6 Check out https://takiaisfobia.blogspot.com/ 
If you are newly suspicious about the safety of the products in your medicine cabinet, there’s a good chance you have Valisure, a tiny laboratory in New Haven, Conn., to thank. Or blame. Tucked away in an unassuming office park, Valisure’s team of about a dozen scientists has over the past five years detected potentially cancer-causing chemicals in widely used medications, hand sanitizers, sunscreens, antiperspirant body sprays, dry shampoos, and—most recently—acne treatments. When Valisure sounds the alarm about a new scary-sounding finding, a flood of headlines, lawsuits, and product recalls often follows. The company is helping to shatter an illusion that some 80% of Americans believe: that the products they buy have been through enough safety testing to be proved not harmful. [time-brightcove not-tgx=”true”]“Most consumers assume that because it’s for sale, it must be safe,” says Teresa Murray, who directs the consumer watchdog office at the nonprofit U.S. Public Interest Research Group (PIRG). “Oftentimes, that’s very much not true.” Despite its nearly $7 billion annual operating budget, the U.S. Food and Drug Administration (FDA) isn’t analyzing every shampoo or supplement on sale at your local drugstore. In fact, the FDA does not approve most cosmetics before they hit shelves—let alone assess how they’ll affect human health after years of regular use. This information vacuum has given rise to a network of nonprofits, consumer-protection groups, and independent scientists dedicated to informing the public about potential hazards lurking in their products. Within this group, Valisure has been uniquely effective at grabbing attention. Its testing has led to product recalls from household-name brands, congressional testimony, and partnerships with big-name organizations like the U.S. Department of Defense and the Kaiser Permanente health system. But Valisure—the underdog that built its reputation as a crusader for public health—has made enemies too. Critics and regulators have denounced its testing methods and the legitimacy of its scientific findings, raising doubts about the very doubts the company has raised. So every time Valisure’s results make the news, Americans are left to figure out how worried they should be. 
The idea for Valisure came not from a grand plan to overhaul decades-old regulatory structures, but from one friend venting to another. In 2015, David Light, a molecular biologist, heard from his friend and former Yale University classmate Adam Clark-Joseph about a problem with his medication. Every so often, Clark-Joseph said, he got a batch that triggered side effects and sent his chronic condition into relapse. He said his doctors mostly shrugged off these incidents as unfortunate quirks of a health care system where supply chains are so complex that quality assurance is difficult. Light remembers being far more shaken than his friend’s physicians. “It was shocking to both of us to realize the FDA’s not testing everything, and retail stores and pharmacies aren’t doing the testing,” he says. “So who’s actually testing the product, as opposed to looking at the paperwork?” Light and Clark-Joseph—now Valisure’s president and head of analytics, respectively—co-founded Valisure in 2015 to fulfill that mission, setting up shop down the road from their alma mater. At first, Valisure quality-tested medications, then sold them through its own online pharmacy. But four years after its founding, Valisure made a name for itself in a splashier way. Read More: A Test Told Me I’m Basically Made of Plastic. You Probably Are Too In September 2019, Valisure’s scientists used a “citizen petition,” which everyday people can use to request action from the FDA, to announce they’d found the probable carcinogen NDMA in every batch of the heartburn medication ranitidine that they tested. Then lawyers brought a slew of lawsuits against GSK and Sanofi, pharmaceutical companies that have sold the popular ranitidine drug Zantac, linking it to clients’ cancers. (Many of these cases have been settled or dismissed.) In April 2020, the FDA asked all makers to pull ranitidine from the market. The FDA has said that the recall was based on its own testing, not Valisure’s. Though FDA tests did find elevated NDMA levels—high enough to trigger a recall—they were much lower than Valisure’s. That’s because Valisure used extreme testing practices, like exposing the drugs to heat, that may have actually produced NDMA, the FDA said in a response to Valisure’s petition. But to the public, a recall is a recall, and Valisure had been the first one to sound the alarm. The scandal boosted Valisure’s reputation; Light still keeps Zantac-branded memorabilia in his office as evidence of his lab’s impact. In 2021, Valisure sold off the pharmacy business to focus on product testing. Mostly—thankfully—this business is a boring one. Valisure’s clients are mainly organizations, like health care systems, that buy lots of medications and want to know what’s in them. About 90% of the time, Light says, this testing is uneventful. But now and then, often operating on their own hunches, his staff finds something concerning. Over the past few years, Valisure has found the carcinogen benzene in a variety of consumer products, including sunscreen, dry shampoo, and acne treatments, leading to major news cycles and, in some cases, product recalls. A range of other groups work in this space. Experts from the Cosmetic Ingredient Review assess the safety of ingredients used in beauty products, with funding from the Personal Care Products Council, an industry trade group. The University of Kentucky’s health care system also performs independent analysis of medications. But unlike Valisure, many of the other groups informing the public about products with questionable safety data—including the Ralph Nader–aligned PIRG, the Silent Spring Institute, Toxic-Free Future, and the Environmental Working Group (EWG)—are nonprofits. Sunscreen is a regular topic of concern for these groups—not necessarily because of benzene contamination, but because of chemical ingredients linked to hormone disruption and cancer—as are things like hair products (some which have also been linked to cancer) and fragrances. These groups have had made splashes too; PIRG was behind the 2018 discovery of asbestos in makeup sold at Claire’s, leading to recalls. “The more we look [at consumer products], the worse it looks,” says Dr. Megan Schwarzman, associate director of the Center for Green Chemistry at the University of California, Berkeley. But, Schwarzman says, it’s not always easy for scientists, let alone the average consumer, to understand what to make of the potential risks raised by these groups. “There’s lead in pigments in lipstick,” Schwarzman says. “If you wear lipstick once a month, it’s probably not a big exposure”—but is wearing lipstick a few times a week enough to cause health problems over years or decades? Is the risk high enough to swear off lipstick altogether? What about other cosmetics? These questions are difficult even for scientists to answer. It’s also near impossible to isolate which chemical exposures, if any, are responsible for health problems, because “we are exposed to [toxins] at generally very low concentrations all the time,” adds Debra Kaden, a toxicologist and principal consultant at the environmental-consulting firm Ramboll. An astounding number of the products in the average American home, for example, contain PFAS “forever” chemicals. Given those realities, consumer-protection groups have their work cut out for them—which is an indictment of the U.S. regulatory system, says Homer Swei, who oversees consumer-safety science at EWG. “It would be great if there was no need for organizations like this,” Swei says. “Why does a third party have to do the heavy lifting for industry and government?” 
The FDA regulates most things that Americans put on and in their bodies, from vaccines to tobacco products, but the scope of its oversight varies depending on the product. Pharmaceutical companies have to conduct complex clinical trials and secure FDA approval before bringing new drugs to market. Meanwhile, the agency’s regulatory structure for cosmetics stems from a law enacted in 1938—long before the average American was using up to a dozen personal-care products, potentially containing more than 100 chemicals in total, every single day. A 2022 law expanded the FDA’s purview over cosmetics—it can now issue a mandatory recall and suspend manufacturing facilities if a serious issue arises—and some states have passed additional laws related to consumer protection. But experts say there are still huge holes in the ways many products are regulated in the U.S. Under the current structure, cosmetics companies can decide what sorts of safety and quality testing they want to do, which often isn’t adequate, Swei says. Brands don’t even have to submit the results of their testing in most cases. And, contrary to popular belief, the FDA rarely orders a recall; more commonly, it requests a voluntary one. Read More: What to Know if Your Doctor Put You on Statins to Lower Cholesterol The FDA is also lenient toward potentially concerning ingredients, compared with regulators in other countries. Since 2009, Europe has required cosmetics makers to submit safety data before selling a new product. In 2023 alone, regulators in the European Union moved to ban 30 chemicals from use in beauty products—more than the FDA has banned from cosmetics in its more than 100 years in existence. Many known or suspected health hazards, like formaldehyde and parabens, are still used in a variety of products sold in the U.S., such as hair treatments and lotions. The FDA has implicitly acknowledged gaps in its approach—like in 2019, when it asked sunscreen manufacturers for more safety data. A spokesperson wrote in a statement that “the agency remains committed to using all available tools to oversee the safety and quality of FDA-regulated products.” The question, for some, is whether Valisure should be one of those tools. Unlike nonprofit groups, Valisure is a business backed by private investors, which means its work has “got to make financial sense,” Light says. Valisure has lobbied for policies that would push companies to pursue the kind of independent testing that’s the bread and butter of its bottom line. “Any increase in the use of independent testing will benefit Valisure as a business,” Light acknowledges. But he maintains it would also be a win for public health. Personal-injury lawyers make a similar argument, saying their fees (routinely 30% to 40% of any damages awarded) serve as a market incentive to hold companies accountable. In court filings, Unilever has also alleged that Valisure is motivated by money. Before filing a citizen petition related to benzene in dry shampoos, Unilever said, Valisure offered to test its products and keep the results confidential if Unilever paid more than $1 million, an offer the company said it declined. And GSK and other companies have questioned Valisure’s relationship with plaintiffs’ attorneys, suggesting the lab works with lawyers to produce test results that will lead to juicy lawsuits. One of the first suits related to Zantac was filed by Light’s brother-in-law, an attorney in Florida. (Light says Valisure’s proposal to Unilever was taken out of context and the lab does not have inappropriate relationships with attorneys, including his brother-in-law, although its scientists sometimes serve as experts in cases.) The FDA has criticisms as well. In a 2022 letter, the agency alleged that Valisure was using inappropriate methods and machinery for its tests. “Third-party testing using unreliable methods produces unreliable data, and decisions based on unreliable data are not sound,” an FDA spokesperson wrote in a statement provided to TIME. Consider Valisure’s recent finding of benzene in benzoyl peroxide acne treatments. For that testing, Valisure scientists analyzed what happened when benzoyl peroxide products were exposed to 122° temperatures for 18 days, conditions that the Personal Care Products Council argued have little real-world relevance. (Light, however, contends the test isn’t so far-fetched: “What if it sits in a warehouse in Florida for two weeks, or sits on a shelf in a store where their air conditioner broke?”) Dr. Philip Landrigan, director of Boston College’s Program for Global Public Health and the Common Good, argues that the public has a right to know about any level of benzene contamination. “We know that it’s a carcinogen, even down to the lowest levels,” he says. Read More: What’s the Best Kind of Sunscreen? But Kaden, the Ramboll toxicologist, says much of the discussion about benzene doesn’t give consumers enough context. In 2022, after Valisure tests revealed benzene in sunscreens, Kaden and a colleague did their own analysis, concluding that people could be exposed to more benzene in the vehicle exhaust they’d inhale walking down a city street than by using a sunscreen contaminated with benzene at the levels Valisure found. Other researchers have also found that people who use sunscreen actually tend to have lower blood concentrations of benzene than nonusers, which suggests these products are not major threats to the general public. Toxin exposure is never a good thing, Kaden says, but “the dose makes the poison.” Groups like Valisure, she says, don’t always make that clear enough in their messaging to the public. Light, however, stands by his lab and its findings. In fact, he seems to enjoy the notoriety that comes with being the guy brave enough to take on the FDA and major brands. Framed articles about Valisure’s bombshell test results line the walls of his office and the lab’s lobby, and he proudly displays the mug he got from a 2023 visit to the White House, where he was invited to talk about product safety. 
Light dabbled in acting as a kid, playing a few parts on Mad TV when he was young. He still has some of that flair for the dramatic, speaking in a booming voice that prompts his publicist to shut his door when he gets going to avoid disrupting the whole office. “Some people like very straightforward spreadsheets and business plans,” Light says. He prefers the spotlight. “I’m an adventurous kind of guy, I guess.” Sometimes, perhaps, too adventurous. During the summer of 2007, while a student at Yale, Light was arrested for firing a pistol into the ceiling of his fraternity house. Authorities reportedly found that Light—who was a gun enthusiast at the time—had numerous weapons, thousands of rounds of ammunition, and chemicals consistent with bomb-making in his room. (Light says the chemicals were not intended for illegal activity and notes that charges related to them were dropped.) He served about six months of a one-year prison sentence and eventually went on to finish his degree at Yale in 2011. “I sincerely regret the events that occurred during my college years,” Light wrote in a statement to TIME. “I take full responsibility for my actions … and since then have made a concerted effort to rebuild my life and contribute positively to society.” How positively Valisure contributes to society is up for debate. The FDA, court system, and trade groups sometimes treat it as a nuisance, arguing its findings scare people without the science to back up the headlines. But the scientists who do similar work maintain that information is power—that even if consumers can’t pinpoint the exact moment at which exposure to benzene or NDMA or parabens becomes dangerous, they have a right to know it’s happening. “It’s up to everybody to decide for themselves the risk-benefit ratio,” Schwarzman says. “When you have the information, you get to do that.” Under the existing regulatory structure, Americans probably wouldn’t get that information without independent labs and consumer-interest groups digging it up. Even finding details about product ingredients and news about product recalls currently requires a little effort on the part of consumers. That may be changing. In addition to state-level efforts, U.S. lawmakers have in recent years introduced legislation that seeks to ban risky chemicals, improve transparency around supply chains and ingredient disclosures, and strengthen oversight of over-the-counter drugs. But for now, consumers are left to operate with imperfect products and limited information, says Kristin Knox, a data scientist at the Silent Spring Institute. In her own life, she’s tried to strike a balance between caution and panic, continuing to use mass-market products while also making tweaks like swapping plastic household goods for glass, choosing unscented products, and using fewer cosmetics. “That there are things you can do that actually reduce your chemical burdens is good news,” she says. “But it’d be even better if the products didn’t have bad chemicals in the first place.” Ultimately, any independent actor, from Valisure to Silent Spring to PIRG, has only so much authority. They can break into the news cycle, which sometimes results in recalls and changes from manufacturers, but they’re not the ones making, selling, and regulating products. Systemic change is required, Knox says, for jobs like hers to become obsolete. “Like most people, I [used to assume], ‘Oh, it’s in the grocery store, it’s been reviewed by the government, it’s safe,’” Knox says. “It would be nice to live in a place where that’s true.” from https://ift.tt/5VFko9n Check out https://takiaisfobia.blogspot.com/ 
Sunscreen is a $10 billion business, with a seemingly endless array of products available for sale. Walk into your local drugstore and you’ll find chemical and mineral formulas in virtually every SPF count and format imaginable, from creams to sprays to sticks. So which one should you throw in your beach bag this summer? Here’s how to choose the right sunscreen, according to dermatologists. [time-brightcove not-tgx=”true”]What’s the difference between chemical and mineral sunscreens?There are two major types of sunscreen: chemical and mineral (also known as physical) formulas. They serve the same purpose—preventing sunburns and other skin damage from the sun’s UV radiation—but they do so in different ways. Sunscreens made from the minerals titanium dioxide and zinc oxide create a physical barrier atop the skin that reflects UV light. Chemical sunscreens, meanwhile, feature active ingredients that sink into the skin and absorb UV rays “like a sponge,” explains Dr. Raman Madan, chief of dermatology at Glen Cove Hospital in New York. In the U.S., these include chemicals such as homosalate, oxybenzone, avobenzone, octinoxate, octisalate, and octocrylene. 
Is chemical or mineral sunscreen better?Many people prefer chemical formulas because they sink into the skin well, whereas mineral sunscreens can leave a chalky white residue. But that residue is a visible signal of these products’ staying power; mineral formulas tend to last longer than chemical sunscreens, says Dr. Abel Torres, chair of the University of Florida College of Medicine’s dermatology department. “If you know you’re going to be on the beach for a long time, mineral may be a better choice because you won’t have to worry about having to reapply it as much,” he says. People with acne-prone skin may also benefit from a mineral sunscreen, since research suggests zinc can help clear blemishes, Torres notes. Those with sensitive skin may also do better with a mineral formula, Madan says, because—unlike chemical sunscreens—these products don’t sink deep into the skin, so “it’s almost impossible to be allergic” to them. For the same reason, people who are skittish about product safety may want a mineral formula. Recent research shows that ingredients used in chemical sunscreens enter the bloodstream after soaking into the skin, and other studies (some conducted in animals) suggest sunscreen chemicals like oxybenzone may be linked to hormone disruption and increased risks of certain cancers. It’s too soon to say exactly if or how absorption of these chemicals affects health, Madan says, but people who are concerned may find peace of mind in mineral formulas. Read More: Backward Walking Is the Best Workout You’re Not Doing There’s broad support for that idea. The U.S. Food and Drug Administration (FDA) has said titanium dioxide and zinc oxide can be generally considered safe and effective, but that there’s not enough data to say the same for chemicals used in sunscreens. (The agency has asked manufacturers to submit additional safety information for analysis.) And all 83 sunscreens verified by the Environmental Working Group, a nonprofit that performs independent analysis of sunscreen safety, are mineral formulas. Still, Torres emphasizes that studies have not proven that chemical formulas are dangerous; they’ve only hinted at potential risks. And there are plenty of known benefits to wearing sunscreen, whether chemical or mineral—most importantly, reducing the risk of skin cancer. So if chemical formulas are the ones you’ll actually use, it’s better to choose those than to go out unprotected. Which SPF is best?Sun protection factor, or SPF, is a measure of how much UV radiation it will take to burn your skin while wearing sunscreen versus while going without. The higher the SPF, the more robust the protection. The FDA recommends choosing a product with an SPF of at least 15, and the American Academy of Dermatology says it’s better to shoot for an SPF of 30 or above. People with fair skin may want to go even higher than that, Madan says—but after a certain point, SPF values offer diminishing returns. An SPF-50 formula offers such strong protection that upgrading to, say, SPF 100 offers only a tiny amount of additional benefit, he says. Read More: The Unsettled—and Unsettling—Science of Lawn Chemicals Just remember that regardless of which SPF you choose, you should reapply after a couple hours in the sun, especially if you’re swimming or sweating heavily. And, in addition to checking the SPF value, the Skin Cancer Foundation recommends choosing a sunscreen that is labeled with the phrase “broad-spectrum protection,” which means it protects against both UVA and UVB rays. UVA rays are responsible for wrinkles and skin aging, while UVB rays are the main cause of sunburns—but both are associated with skin cancer. Is sunscreen best as a spray, lotion, or stick?Sprays, sticks, and other formats are convenient, but Madan recommends a good old-fashioned cream if you have the choice. “It goes onto the skin a little bit thicker, so patients get more coverage out of a lotion,” he says. Research backs up that point. Studies have shown that people often don’t apply enough sunscreen when they use aerosol products, since the spray can be easily carried away by the wind and many formulas are diluted by propellants and other ingredients. Using a spray also introduces the possibility of inhaling potentially harmful substances, particularly if applied directly to the face. But something is always better than nothing, Madan says—so if a spray is all you have, use that. The one exception? The FDA has said it needs more data to prove that sunscreen powder is effective, so Madan typically recommends patients steer clear of those products in favor of tried-and-true formulations. from https://ift.tt/qUgHcDr Check out https://takiaisfobia.blogspot.com/ 
In March 2023, the Japanese medical authorities announced that the new weight loss drug Wegovy—which was in staggering demand across the world, causing shortages everywhere—had been approved to treat obesity in their country. It sounded, at first glance, like great news for Novo Nordisk, the company that makes Ozempic and Wegovy. But industry outlet the Pharma Letter explained that this would not in fact turn out to be much of a boost. They predicted that these drugs would dominate the market in Japan, but that won’t mean much, for a simple reason: there is almost no obesity there. Some 42% of Americans are obese, compared with just 4.5% of Japanese people. Japan, it seems, is the land that doesn’t need Ozempic. [time-brightcove not-tgx=”true”]I wondered how this could be, and if the answer might offer me a way out of a dilemma that was obsessing me. Several months before, I had started taking Ozempic, and I was traveling all over the world to interview the leading experts on these drugs to research my new book, Magic Pill: The Extraordinary Benefits and Disturbing Risks of the New Weight-Loss Drugs. The more I discovered, the more torn I became. I had learned there are massive health benefits to reversing obesity with these drugs: for example, Novo Nordisk ran a trial that found weekly injections reduced the risk of heart attack or stroke by 20% for participants with a BMI over 27 and a history of cardiac events. But I also saw there are significant risks. I interviewed prestigious French scientists who worry the drugs could cause an increase in thyroid cancer, and eating disorders experts who worry it will cause a rise in this problem. Other experts fear it may cause depression or suicidal thoughts. These claims are all fiercely disputed and debated. I felt trapped between two risky choices—ongoing obesity, or drugs with lots of unknowns. So I went to Japan, to discover: how did they avoid this trap? My first assumption was that the Japanese must have won the genetic lottery—there had to be something in their DNA that makes them stay so slim. But in the late 19th and early 20th century, large numbers of Japanese workers migrated to Hawaii and they have now been living on the island for four generations. They are genetically very similar to the Japanese people who didn’t leave. It turns out that after 100 or so years, Japanese Hawaiians are now almost as overweight as the people they live among. Some 18.1% of them are obese, compared to 24.5% of Hawaiians overall. That means Japanese Hawaiians are four times more likely to be obese than people back in Japan. So something other than genes explains Japan’s slimness. But what? I glimpsed part of the explanation when I went to the Tokyo College of Sushi & Washoku, to interview the president Masaru Watanabe, who I also spoke with on Zoom on another occasion. He had agreed to cook a meal for me with some of his trainees, and to explain the principles behind it. He told me: “The Japanese cuisine’s [core] feature is simplicity. For us, the simpler, the better.” He began to make a typical Japanese meal, the kind people were eating all over the country that lunchtime. He and his chefs grilled a mackerel, boiled some rice, made some miso soup, and prepared some pickles. “We don’t traditionally eat meat a lot. We are an island country. We appreciate fish.” As the mackerel was grilled, I watched as various oils and fats leeched out. Even more importantly, Masaru explained, this was an illustration of one of the crucial principles of Japanese cooking. Western cooking, he said, is primarily about “adding.” To make food tasty, you add butter, lemon, herbs, sauces, all sorts of chemicals. “But the Japanese style is totally the opposite.” It’s “a minus cuisine.” It is about drawing out the innate flavor, “not to add anything extra,” he said. The whole point is to try “to make as much as possible of the ingredients’ natural taste.” To Japanese cooks, less is more. He also said Japanese meals have very small portions, but more of them—five in a typical meal. Before we started to eat, Masaru explained the Japanese principles of eating. The first thing I had to learn was “triangle eating.” All my life, when I was eating a meal with different components, I would mostly eat them sequentially—start the soup, finish the soup; start the salad, finish the salad; start the pasta, finish the pasta. “In Japan, this is regarded as really weird,” he said. “It’s a rude way of eating.” A meal like this should be eaten in a triangle shape. “First, drink the soup a little bit, then go to the side dish—one bite. Then try the rice, for one bite. Then the mackerel—again, a single mouthful. Then go back and have another taste of the soup,” he said. “This is also the key to keep you healthy … Keeping the balance, so you don’t eat too much.” The second thing we had to learn is when to stop. In Japan, you are taught from a very early age to only eat until you feel you are 80% full. It takes time for your body to sense you’ve had enough, and if you hit a sense of fullness while you are still eating, then you’ve definitely had too much. I ate nothing but Japanese food like this on my trip, and three days in, I began to experience an odd mixture of hope and humiliation. I felt healthier and lighter, but I also thought—the Japanese people have built up a totally different relationship to food over thousands of years, in ways we can’t possibly import. So I was surprised to learn that most of Japan’s food culture was invented very recently—in living memory, in fact. Barak Kushner, who is professor of East Asian History at the University of Cambridge, told the writer Bee Wilson, for her book First Bite, that until the 1920s, Japanese cooking was just “not very good.” Fresh fish was eaten only once a week, the diet was dangerously low in protein, and stewing or stir-frying were not much of a thing. Life expectancy was a mere 43. It was only when Imperial Japan was creating an army to attack other parts of Asia that a new food culture began to be invented, quite consciously, to produce healthier soldiers. After the defeat of Japan in the Second World War, when the country was in ruins, the new democratic government stepped up this transformation. To find out how Japan created a radically different food culture, I arrived at Koenji Gakuen School with my translator on a stiflingly hot September morning. It’s a typical school for kids aged from five to 18 in a middle-class neighborhood in Tokyo. We were greeted near the entrance by Harumi Tatebe, a woman in her early 50s, who had been the nutritionist there for three years. As we walked through the corridors, kids waved at her affectionately, and shouted her name, eager to know what they were having for lunch that day. By law, Harumi said, every Japanese school has to employ a professional like her. It took her three years to qualify, on top of her teaching degree, and she explained that in this position, you have several important roles to play. You design the school meals, in line with strict rules stipulating that they must be fresh and healthy. You oversee the cooking of the meals. You then use these meals to educate the children about nutrition. Then you educate their parents on the same topic. 
Harumi told me that today’s meal consisted of five small portions: some white fish, a bowl of noodles with vegetables, milk, some sticky white rice, and a tiny dollop of sweet paste. All the kids eat the same meal, and packed lunches are forbidden. No processed or frozen food ever goes into any of the meals here. “We start from scratch,” she said. “It’s all about nutrition … Sometimes with frozen food, they use a lot of artificial additives.” Once the meal was ready, Harumi carried a tray over to the office of the school’s head, Minoru Tanaka. It is a legal requirement that the principal of each school ensures lunches meet nutritional guidelines. It’s also customary for principals to have the same lunch as the kids and to eat it first, to make sure it’s safe, nutritious, and delicious. He rolled up his sleeves and dug in. After a moment, he nodded approvingly. Before they began to eat, a child stood at the front of the class and read out what today’s meal was, which part of Japan it came from, and how the different elements are good for your health. She then said “Meshiagare!,” the Japanese equivalent of “bon appétit,” and everyone applauded. While the kids were eating, Harumi held up some colored ropes. Each one represented a different kind of food you need to be healthy. On this day, she held up the yellow rope, representing carbs, and asked what they do for your health. A child yelled: “Give you energy!” She held up the red rope, representing calcium, and a child yelled that it makes your bones stronger. As she went though the food groups, she tied each rope together, to show that in combination they make a healthy meal. “Through the school lunches, we explain the food itself,” the principal, Mr. Tanaka, told me. As I walked around, I had a nagging sense that there was something unusual about this place. But it was only after a few hours that I realized what it was. There were no overweight children. None. My translator and I walked from class to class, asking the kids what they most liked to eat. The first child I spoke to, a 10-year old girl, said: “I like green vegetables, like broccoli.” One 11-year old-boy told me he loves rice because “the rice has protein. If you eat balanced food every meal, then you have a very strong body,” and he flexed his tiny biceps, and giggled. I asked my translator: Is this a joke? Are they trolling me? A bunch of 10-year-olds, telling me how much they love broccoli and rice? But most of the Japanese people I discussed this with were puzzled to see that I was puzzled. We teach kids to enjoy healthy food, they explained. Don’t you? Up until this point, I had seen aspects of Japan’s approach toward health that seemed totally admirable. But next, I saw something that left me with mixed feelings. In 2008, the Japanese government noticed that obesity was slightly rising. So they introduced the “Metabo Law,” which was designed to reduce the negative consequences of a large waistline. The law contained a simple rule. Once a year, every workplace and local government in Japan has to bring in a team of nurses and doctors to measure the waistline of adults between ages 40 and 74. If the measurements are above a certain level, the person is referred to counseling, and workplaces draw up health plans with employees to lose weight. Companies with fattening work forces can face fines. I couldn’t imagine how this could possibly work, so I went to see it in practice. A company called Tanita agreed to let me talk to their employees about it, and to see the measures they have put in place. They make vegan food, healthy meal replacements, and exercise equipment, so they are especially keen to promote a healthy Japan. Different companies stay in line with the Metabo Law in different ways, and Tanita is at the most enthusiastic edge. The first person I met with was Junya Nagasawa, the company’s boss. He is a handsome 57-year-old who consistently comes top of the company’s walking league table, with nearly 20,000 steps a day. When the Metabo Law came into force, he told me, there was a sudden demand from companies for technologies that could help them monitor their employee’s health and find ways to improve it, so Tanita designed video screens and health surveillance systems. Everyone in the company wears a watch that tracks how many steps they walk a day, and when you arrive at work every day, it tells you how much you’ve walked—and how much your colleagues have walked. You are encouraged to post photos of all your meals, and pledges for how you’ll improve your health—which are, again, visible to the entire company. Nagasawa told me these measures meant he started to walk much more. “It’s not difficult to walk, but it’s very difficult to make the time,” he said. Now, he gets up earlier, and gets off the subway four stops sooner to walk the rest of the way. “I had to be the role model,” he said. I spoke with some of his employees. The 33-year-old Yusuke Nagira told me he came to work here straight from university, and he had never done anything to look after his health up to that point. “I would eat whatever I wanted to eat and didn’t exercise at all. That was my lifestyle.” But he noticed from logging his weight that he was putting on pounds, and he was conscious of the looming annual health checks. So he made some changes. Before, “when I was watching TV, I would usually eat junk food or snacks.” He cut them out completely. And “when I go out to other places, I try not to use trains or drive, but walk.” Knowing he’ll be accountable helps him, he said. I heard this again and again from the workers. I told all the Japanese people I talked to that if you tried this in the U.S. or Britain, people would be outraged and burn down their offices. They invariably looked puzzled, and asked me why. I said that people would feel like it was not their employer’s business what they weighed, and that it was a monstrous intrusion of their privacy. Most of them nodded politely, said nothing, and looked at me like I was slightly crazy. Nagira said simply: “Being fat is not good.” I felt like I was communicating across a cultural chasm. Whatever you think of its ethics, the Metabo Law does seem to be—along with Japan’s other measures—having an impact. Its obesity rate is currently the lowest level in the rich world. As I traveled across the country, I began to see what you gain if you live in the Japanese style. Every morning around 7 or 8 a.m., in parks across Japan, elderly people gather in groups and exercise together. You can watch people in their 80s and 90s dancing or doing yoga. Japanese people live longer than anyone else on earth. On average, men live to be 81, and women reach 88. Even more importantly, they remain healthy for longer. 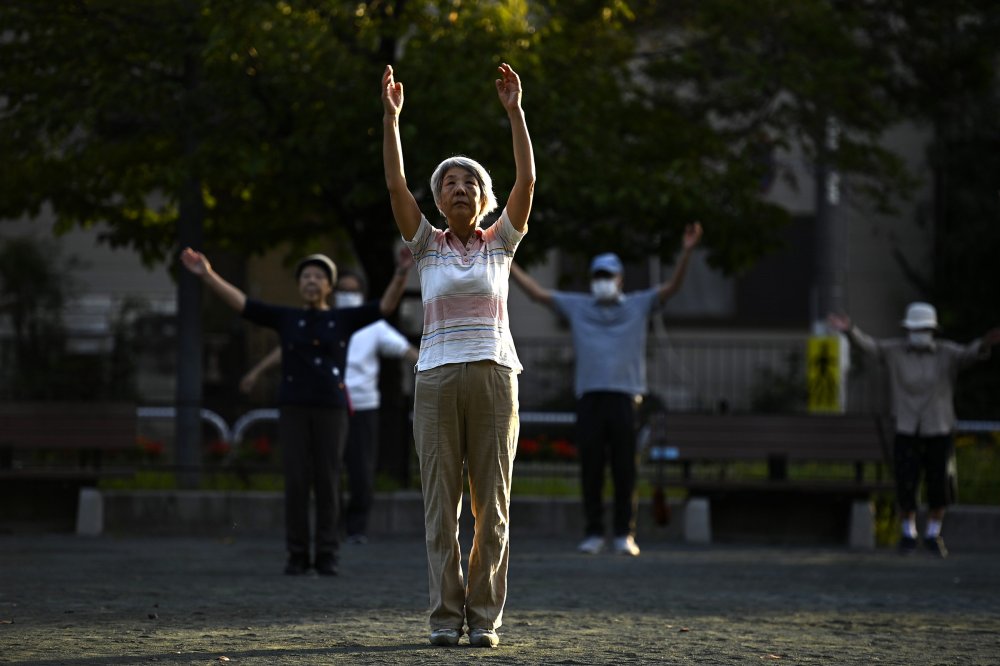
I went to Okinawa, an archipelago of islands in the far south of the country, to track down somewhere that sounds almost mythical—a place that is described by local Japanese authorities as the village with the oldest population in the world (though another village in Japan has recently been declared the oldest in the country). By the side of a lush tree-covered mountain, we drove into Ogimi. It has 215 households, and 173 people there are aged 90 or older. The people who live here have had hard lives—they were mostly poor farmers, and during the Second World War, in the space of just three months, roughly a third of the population was killed during the Battle of Okinawa. In their little concrete community center, some of the very elderly residents were arriving, looking forward to catching up with each other, playing games and exercising together. The first person we met was Matsu Fukuchi, a 102-year-old woman, who had walked to the center from her home, slowly but without a stoop, holding on to a cane. Her eyes watched us with curiosity. She said she took a lot of pleasure in life. “I get together with my grandchildren and have fun, and dance. I love to dance.” Some traditional Okinawan music began to play, and Matsu put on a brightly colored kimono. Then slowly, carefully, joyfully, she stood up, and began to dance. She moved her hips gently in time with the music, and the other women matched her rhythm, waving their arms. She looked toward me, beaming. As I watched these centenarian women move with the music, I realized--this is what this whole journey has been about. While she waved her 102-year-old hips in my direction, I thought: This is the potential prize here, if we can solve the obesity crisis. More life. More health. More years of joy. Suddenly, the sheer artificiality of the obesity crisis seemed clear to me, more than at any other point on this journey. It is created by the way we live. It should be possible, therefore, to un-create it. But how can we do that? At first glance, the gap between us and the Japanese seemed unbridgeable. But then I thought about something from my own childhood. If I could take a young person back to the Britain or the U.S. of the 1980s, they would be astonished by one habit. People smoked cigarettes everywhere. They smoked in restaurants. They smoked on planes. They smoked on game shows. When you went to see the doctor, he would smoke while he examined you. (I’m not kidding: I remember this happening.) If you had said to people then that within a generation, smoking would come to look like a thing of the past, we would not have believed you. In 1982, for example, 33% of men and women in the Minnesota Heart Survey were smokers. Today, only 12% of the U.S. population smokes cigarettes, and it’s falling further. I had asked Masaru Watanabe, the Japanese chef, if it was possible for Westerners to become like the Japanese. “I hope so,” he said. “I definitely think so,” he clarified. I have traveled to many different parts of the world where they have begun changes that bring us closer to Japanese levels of health. In Mexico, they introduced a sugary-drinks tax. In Amsterdam, they restricted sugary drinks from schools and gave overweight kids personalized health coaches, slashing childhood obesity by 12% between 2012 and 2018 (though it has ticked up since). In various U.S. cities, there are “food is medicine” programs. There are dozens of social changes we could make that would reduce the huge forces driving up obesity. None of this, in the short term, can get me out of the dilemmas posed right now by the new weight loss drugs. In the U.S. and other rich countries (with the exception of Japan), many of us will have to weigh the risks of continuing to be overweight, against the risks of taking these drugs. I am continuing to take Wegovy, but with a heavy sense of concern about the potential dangers. Yet Japan shows us that if we make the right social changes now, we can free our children of this dilemma. If we look East, we will realize we don’t have to be trapped in the choice between Wegovy versus weight gain forever. Adapted from MAGIC PILL: The Extraordinary Benefits and Disturbing Risks of the New Weight-Loss Drugs by Johann Hari. Copyright © 2024 by Johann Hari. Published in the United States by Crown, an imprint of the Crown Publishing Group, a division of Penguin Random House LLC. from https://ift.tt/aH2qWXw Check out https://takiaisfobia.blogspot.com/ 
More than 321,000 children in the U.S. lost a parent to a drug overdose from 2011 to 2021, an alarming figure that shows the nation’s obligation to “comprehensively address the needs of individuals, families and communities” when tackling the growing overdose crisis, experts say. [time-brightcove not-tgx=”true”]A new study published Wednesday in the medical journal JAMA Psychiatry found that the rate of children who lost a parent to an overdose more than doubled in that decade span, jumping from 27 to 63 children per 100,000. In total, the study estimates that 321,566 children in the U.S. lost a parent to a drug overdose in that time span. And while the rates of loss increased consistently each year across all demographics examined in the study, people of color were disproportionately affected by this trend. The highest number of deaths were among white parents, but children of American Indian or Alaska Native parents experienced the highest rates of loss, the study found. Children with young Black parents between the ages of 18 and 25 experienced the highest increase in the rate of loss each year. The study was conducted by researchers from the Substance Abuse and Mental Health Services Administration (SAMHSA), the U.S. Centers for Disease Control and Prevention (CDC), and the National Institute on Drug Abuse (NIDA). Nearly 650,000 people between the ages of 18 and 64 died of a drug overdose from 2011 to 2021, but this was the first national study to estimate the number of children who lost a parent in that span, according to a press release about the study from the National Institutes of Health (NIH). Researchers used data from the National Surveys on Drug Use and Health and the CDC National Vital Statistics System to conduct the study. “It is devastating to see that almost half of the people who died of a drug overdose had a child,” Nora Volkow, the director of NIDA, said in the press release. “No family should lose their loved one to an overdose, and each of these deaths represents a tragic loss that could have been prevented.” Researchers said that the study highlighted the need for holistic health care to treat people who struggle with substance abuse and the importance of providing prevention resources to help families break generational cycles of substance abuse. “These data illustrate that not only are communities of color experiencing overdose death disparities, but also underscore the need for responses to the overdose crisis moving forward to comprehensively address the needs of individuals, families and communities,” Miriam Delphin-Rittmon, the leader of SAMHSA, said in the NIH’s press release. from https://ift.tt/zbldXLI Check out https://takiaisfobia.blogspot.com/ 
Presidential candidate Robert F. Kennedy Jr. said he suffered memory loss and severe brain fog more than a decade ago, potentially related to a parasite in his brain, according to the New York Times. In a 2012 deposition reviewed by the Times, Kennedy said a worm “got into my brain and ate a portion of it and then died.” He said the cognitive issues later resolved. Around the same time, the Times reports, Kennedy was also diagnosed with mercury poisoning, which can also result in cognitive issues. [time-brightcove not-tgx=”true”]Though they sound like something straight out of a horror movie, parasites can and do affect the human brain. Here’s what to know. How do parasites get into the brain?According to the Times‘ reporting, Kennedy said he did not know which type of parasite affected him, but experts told the Times it likely came from the larvae of a tapeworm sometimes found in pork. People can ingest a tapeworm’s eggs by eating contaminated food or water, resulting in the parasitic infection cysticercosis—which is called neurocysticercosis when it affects the brain. Most often, people contract neurocysticercosis not directly from eating pork, but through exposure to fecal contamination, says Scott Gardner, curator of the Manter Laboratory of Parasitology at the University of Nebraska-Lincoln. If someone eats undercooked pork carrying a tapeworm, they may later pass the worm’s eggs through their feces. If the affected person does not properly wash their hands after using the bathroom, they may spread the worm’s tiny eggs to household surfaces or to food and water, potentially leading people to ingest them and get sick, according to the U.S. Centers for Disease Control and Prevention (CDC). When the eggs hatch and larvae get into tissues like the brain, they form cysts there. Read More: Ticks Carry More Diseases Than Lyme. Here’s What You Need to Know Neurocysticercosis is rare in the U.S., but it is more common in parts of Asia and Latin America, says Gardner. As of 2017, the U.S. National Institute of Allergy and Infectious Diseases estimated that only about 1,500 cases were diagnosed in the U.S. each year. A 2012 study estimated its mortality rate to be around 0.06 deaths per 1 million people in the U.S. Toxoplasma gondii is another far more common parasite that can affect the human brain, resulting in the infection toxoplasmosis. It can be spread via exposure to feline feces, as well as eating undercooked meat or shellfish or drinking contaminated water, the CDC says. The CDC estimates that up to 40 million people in the U.S. carry the parasite, though many don’t know it. How dangerous are brain parasites?Surprisingly, brain parasites don’t always cause serious issues, says Tajie Harris, an associate professor of neuroscience at the University of Virginia School of Medicine who has studied brain parasites. “We acquire a lot of infections that we never really notice or attribute to these viruses or parasites that do end up in our brains for the long-term,” she says. “Most of them go into this dormant state and cause us no problems in our lifetime.” Harris’ research, for example, has shown that the brain launches such an effective immune response against T.gondii that many people never develop toxoplasmosis symptoms. When people do experience symptoms, which can be treated with antiparasitic medications in combination with antibiotics, they may develop flu-like muscle aches and swollen glands. Severe toxoplasmosis, which is most common among infants and people who are seriously immunocompromised, can result in damage to the brain, eyes, and other organs. Some studies have also linked the infection to mental-health issues, although Harris says that science is less settled. Read More: The New Vaccines to Get in 2024 Neurocysticercosis can also remain dormant for some time. People do not typically develop symptoms until cysts caused by the parasite die, which can take months or even years, the CDC says. Symptoms can include headaches, seizures, confusion, and difficulty focusing and balancing. In serious cases, the condition can lead to excess fluid around the brain, which may be fatal. Typically, neurocysticercosis can be treated with antiparasitic drugs, sometimes used in combination with anti-inflammatory medications and surgery. Dr. Michael Schulder, professor and vice chair of neurosurgery at Northwell Health in New York, says the symptoms Kennedy apparently suffered, including memory loss and brain fog, are not typical for neurocysticercosis and would likely be associated with a “particularly large cyst that put pressure on the brain.” The parasite also does not eat the brain, he clarifies. If it did, the sufferer would have permanent damage. “It may not be gross damage that would prevent you from leading an independent life,” Schulder says, “but it would certainly prevent you from functioning at 100%.” How can I prevent brain parasites?Good hygiene and food preparation practices are important. Health authorities emphasize the importance of thoroughly washing your hands after using the bathroom, changing a child’s diaper, or handling a cat’s litter box. And make sure to wash fresh produce and cook meat to a safe temperature, which for pork is at least 145°F. But, Schulder says, the average person shouldn’t spend much time worrying about parasitic brain infections—particularly not rare ones like neurocysticercosis. “In a society where public health and public hygiene measures are typically taken, and we have a Food and Drug Administration that oversees production of food and how it’s made available to the public,” he says, brain-invading parasites shouldn’t be a major concern. from https://ift.tt/QwN7blu Check out https://takiaisfobia.blogspot.com/ 
(BANGKOK) — The prime minister of Thailand, the first country in Asia to legalize cannabis two years ago, said Wednesday that he wants to outlaw the drug again amid concerns that the lack of regulation had made it available to children and increased crimes. Prime Minister Srettha Thavisin wrote on the social media platform X that he asked the Health Ministry to amend its list of narcotics to again include cannabis, and issue new rules to allow its use for medical purposes only. [time-brightcove not-tgx=”true”]Srettha also ordered local authorities to suppress criminal activities linked to the illegal drug trade and demanded to see progress within 90 days. After cannabis was decriminalized in 2022, it was initially said that it would be allowed only for medicinal use, but in practice the market was unregulated. It has prompted public backlash and concerns over misuse and crime. Decriminalization was spearheaded by the Bhumjaithai Party, whose stronghold is in the impoverished northeast where it promised farmers cannabis would be a new cash crop. In the 2023 elections, all major parties — including Bhumjaithai — promised to restrict cannabis for medical use. Cannabis advocates and entrepreneurs have opposed a radical rollback, which they claimed would be damaging to the economy. Legal cannabis has fueled Thailand’s tourism and farming sectors and spawned thousands of cannabis retails ranging from shops, trucks to market stalls all over the country. from https://ift.tt/Fz6eUdC Check out https://takiaisfobia.blogspot.com/ 
(NEW YORK) — All dogs coming into the U.S. from other countries must be at least 6 months old and microchipped to help prevent the spread of rabies, according to new government rules published Wednesday. The new rules require vaccination for dogs that have been in countries where rabies is common. The update applies to dogs brought in by breeders or rescue groups as well as pets traveling with their U.S. owners. [time-brightcove not-tgx=”true”]“This new regulation is going to address the current challenges that we’re facing,” said Emily Pieracci, a rabies expert at the Centers for Disease Control and Prevention who was involved in drafting the updated regulations. The CDC posted the new rules in the federal register on Wednesday. They take effect Aug. 1 when a temporary 2021 order expires. That order suspended bringing in dogs from more than 100 countries where rabies is still a problem. The new rules require all dogs entering the U.S. to be at least 6 months, old enough to be vaccinated if required and for the shots to take effect; have a microchip placed under their skin with a code that can be used to verify rabies vaccination; and have completed a new CDC import form. There may be additional restrictions and requirements based on where the dog was the previous six months, which may include blood testing from CDC-approved labs. The CDC regulations were last updated in 1956, and a lot has changed, Pieracci said. More people travel internationally with their pets, and more rescue groups and breeders have set up overseas operations to meet the demand for pets, she said. Now, about 1 million dogs enter the U.S. each year. Dogs were once common carriers of the rabies virus in the U.S. but the type that normally circulates in dogs was eliminated through vaccinations in the 1970s. The virus invades the central nervous system and is usually a fatal disease in animals and humans. It’s most commonly spread through a bite from an infected animal. There is no cure for it once symptoms begin. Four rabid dogs have been identified entering the U.S. since 2015, and officials worried more might get through. CDC officials also were seeing an increase of incomplete or fraudulent rabies vaccination certificates and more puppies denied entry because they weren’t old enough to be fully vaccinated. A draft version of the updated regulations last year drew a range of public comments. Angela Passman, owner of a Dallas company that helps people move their pets internationally, supports the new rules. It can especially tricky for families that buy or adopt a dog while overseas and then try to bring it to the U.S., she said. The update means little change from how things have been handled in recent years, she said. “It’s more work for the pet owner, but the end result is a good thing,” said Passman, who is a board member for the International Pet and Animal Transportation Association. But Jennifer Skiff said some of the changes are unwarranted and too costly. She works for Animal Wellness Action, a Washington group focused on preventing animal cruelty that helps organizations import animals. She said those groups work with diplomats and military personnel who have had trouble meeting requirements, and was a reason some owners were forced to leave their dogs behind. from https://ift.tt/NbKiplq Check out https://takiaisfobia.blogspot.com/ 
Jess, 38, has lost 75 pounds since she started taking Wegovy last year. She’s thrilled with the results—in addition to losing weight, her blood work and sleep apnea have improved—but the changes to her life and body feel too fraught to talk about with her friends, who want nothing to do with her weight loss. Years ago, Jess, who asked to use only her first name for privacy, and her friends embraced the principles of the Health at Every Size movement, which fights against anti-fat bias and argues that weight is not an accurate indicator of health. But last summer, despite her support for that school of thought, Jess decided that she wanted to lose weight to feel better in her body. When she mentioned that decision to her friends, “they told me, ‘We have no interest in this conversation. We do not want to discuss this with you. We don’t agree with your choice,’” she remembers. “I respect their boundaries, but it’s been difficult not to share certain milestones with them or even talk about day-to-day things. It’s been kind of sad and lonely.” These days, she only discusses her weight loss with her doctor and her husband. [time-brightcove not-tgx=”true”]Weight loss has always been a fraught topic. But it’s especially complex to talk about in 2024, as body-positivity movements collide with the popularity of drugs like Ozempic, Wegovy, and Zepbound. Largely because of these medications, weight loss is all over the news and social media—and nobody, it seems, knows exactly how to feel or talk about that. “It’s such a sensitive topic because we can hide so much about our lives,” says Rachel Goldman, a New York City-based clinical psychologist who specializes in weight management and has consulted for a health care company that prescribes anti-obesity medications. “But if you’re gaining weight or losing weight, somebody’s going to see it.” Read More: 6 Compliments That Land Every Time Even many health care providers, who talk about sensitive topics all day long, find weight loss a uniquely challenging subject, says Charlotte Albury, a medical anthropologist at the University of Oxford in the U.K. who studies communication in health care settings. That’s in part because there’s so much “shame and blame and stigma that society perpetuates around obesity,” she says, and in part because “lots of clinicians feel very undertrained in talking about obesity.” If clinicians feel undertrained, where does that leave the rest of us? When it comes to societal opinions about weight loss, the pendulum has swung far in only a couple of decades. Not too long ago, nearly all of mainstream culture treated weight loss as aspirational. Now, although weight stigma is still a significant issue in the U.S., the weight-loss discussion includes far more dissenting voices than it once did. In March, when Oprah Winfrey aired a (mostly positive) television special about GLP-1 drugs, the technical name for medications like Ozempic and Wegovy, she alluded to the myriad opinions about modern weight loss. “For people who feel happy and healthy in celebrating life in a bigger body and don’t want the medications, I say, ‘Bless you,’” Winfrey said. “For all the people who believe diet and exercise is the best and only way to lose excess weight, bless you, too, if that works for you. And for the people who think that this could be the relief and support and freedom…that you’ve been looking for your whole life, bless you, because there is space for all points of view.” Often, though, those points of view butt up against one another. Some people trying to lose weight, like Jess, feel conflicted, both glad that society is taking a hard look at diet culture while also hesitant to say anything positive about weight loss for fear of being accused of fatphobia. (A recent New York Times article highlighted the tricky situation some body-positivity influencers face when they get smaller, with their followers sometimes viewing weight loss as a “betrayal.”) Margit Berman, a Minnesota-based psychologist who fights against diet culture in her practice, says some of her clients also hide that they’re using GLP-1 drugs for diabetes, the condition for which Ozempic and Mounjaro are approved, because they’re afraid of being blamed for being sick because of their weight. Other people apparently don’t feel as conflicted. Demand for GLP-1 medications is booming, with some projections estimating that around 10% of the U.S. population will be using one of these drugs by 2030. And while many people use these medications based on the advice and prescription of a physician, some are so eager to drop pounds that they’re willing to buy drugs like Ozempic from compounding pharmacies, med spas, Internet companies, and other questionable sources. Read More: Why Is It So Bad to Pop a Pimple? Then there are people who are open about wanting to lose weight, but only the old-fashioned way—that is, with diet and exercise, rather than “cheating” by using medications. In a 2024 Pew Research Center poll, about half of U.S. adults said drugs like Ozempic are good weight-loss options for people with obesity, while roughly as many either said they’re not good options or weren’t sure what to think. Similar trends are playing out among physicians. Some doctors talk about GLP-1s as revolutionary treatments for the chronic disease of obesity, lauding not only their ability to help people shed roughly 20% of their body weight but also their benefits for cardiovascular health. Goldman adds that anti-obesity medications may help reduce weight stigma, because they may help people see obesity just like any other disease requiring treatment. Other doctors, meanwhile, argue GLP-1s come with significant drawbacks—side effects include GI issues and, possibly, increased risk of thyroid tumors, and most people gain back the weight they lost if they stop taking them—and help perpetuate harmful beliefs that smaller bodies are automatically better and healthier. Berman thinks GLP-1 drugs contribute to “magical thinking” rooted in anti-fat bias: that weight loss is the easiest way to a good life. Dr. Silvana Pannain, director of the University of Chicago Medicine’s weight-loss program and an advisor to companies that make GLP-1 drugs, thinks that disagreement has probably always been there, but social media and the buzz about GLP-1 drugs are now amplifying it. “It’s not necessarily a different way of thinking, but that more people feel the right to voice their opinion about obesity,” Pannain says. Read More: How Doctors Inadvertently Fat-Shame Kids Berman, however, has noticed a change. When she started speaking out against weight-loss culture in the early 2000s, “People looked at me like I had three heads,” she remembers. “The culture was that fat hatred was acceptable, and everyone should be trying to lose weight. There wasn’t the same [weight-positive] countercultural stream that there is now.” Still, thin-preference remains dominant in the U.S. Even as more people outwardly embrace body positivity and acknowledge that weight loss is a complex topic, a significant percentage of U.S. adults say they want to slim down--as of 2023, about 55% of women and 47% of men, roughly the same numbers as a decade ago. Almost 30% of U.S. adults said in a 2023 study that their worry about having obesity has increased since the COVID-19 pandemic, with about 6 million saying they’d considered surgery or medication in recent years. Americans still want to lose weight; they just may not feel comfortable announcing that intention proudly anymore. Jess, the woman using Wegovy, says all she wants is to land on a middle ground, somewhere between rabid diet culture and feeling shunned by her friends because of her GLP-1 prescription. “We need to somehow neutralize” the idea of weight loss, removing the moral baggage attached to either deciding to drop pounds or deciding not to, she says. “In a world where a lot of us believe that our body is our choice, this is another one of those things that should go into that category.” from https://ift.tt/CcBmMie Check out https://takiaisfobia.blogspot.com/ |
Authorhttps://takiaisfobia.blogspot.com/ Archives
April 2023
Categories |
 RSS Feed
RSS Feed
